Trump’s Latest Executive Orders: Head Fakes and Head Games
[NB: Check the byline, thanks! /~Rayne]
Before we look at the craptacular bullshit Trump and his henchmen pulled over on major media outlets Friday and Saturday, let’s take a look at what needs urgent resolution.
A COVID-19 patient was evicted from her home while she was still recovering. The ownership of the home is in question yet she was booted out, still struggling to breathe while all her belongings are tossed out on the lawn.
This is likely not the only example like this. The article above notes there have been 9,000 eviction filings in the Memphis, Tennessee area as of June. How many are there today?
How many eviction filings are there across the entire country?
Bloomberg reported as much as a third of renters don’t think they will be able to make August rent payment:
Renters across America are wading into unknown territory. With the lapse of the federal moratorium on evictions that expired July 31 and the end of the $600 per week boost to unemployment benefits, a recent survey reveals the breadth of financial uncertainty now plaguing Americans.
An estimated 27% of adults in the U.S. missed their rent or mortgage payment for July, according to a nationwide survey conducted by the U.S. Census Bureau weekly over the last three months. Among renters alone, just over one-third (34%) said during the waning days of July that they had little to no confidence that they could make their August rent payment, a stark measure of the ongoing economic devastation for households stretched to the brink by coronavirus pandemic.
There were 43 million renters in 2019. If that number hasn’t changed we could be looking at nearly 15 million evictions within the next month.
This doesn’t include homeowners who haven’t or may not be able to make their mortgage payments.
This is a massive crisis which is kicking off slowly thanks to the GOP Senate refusing to negotiate with its HEALS Act to meet the House Democrats’ HEROES Act which was passed in May and has been ready to go since then.
Given 51 million Americans were unemployed by mid-July and many had difficulty collecting unemployment compensation on a timely basis, the scale of homelessness we are about to see because Trump and the GOP are such massively useless asshats will make the 2008 crash look like nothing.
~ ~ ~
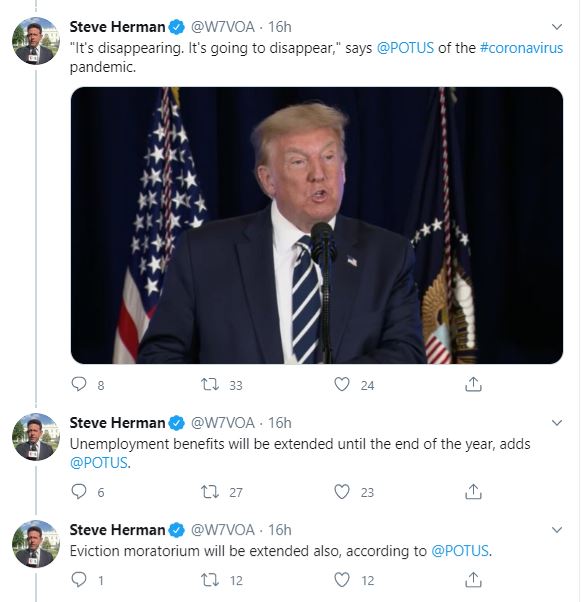
At his Bedminster golf club Friday evening — in front of club members who didn’t wear masks in spite of New Jersey’s emergency orders — Trump threw out teasers about executive orders to help Americans:
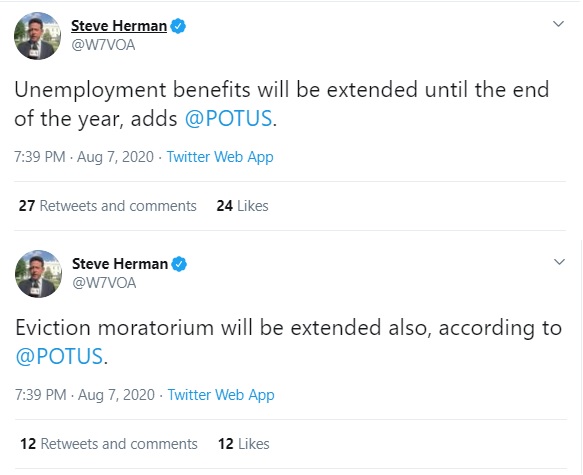
These are Steve Herman’s live tweets capturing the event.
Many major media outlets reported Trump’s comments without any skepticism.
Just before 5:00 p.m. Saturday, Trump signed so-called executive orders. Again, major media reported this straight without any pushback, as Josh Benton noted in his feed:
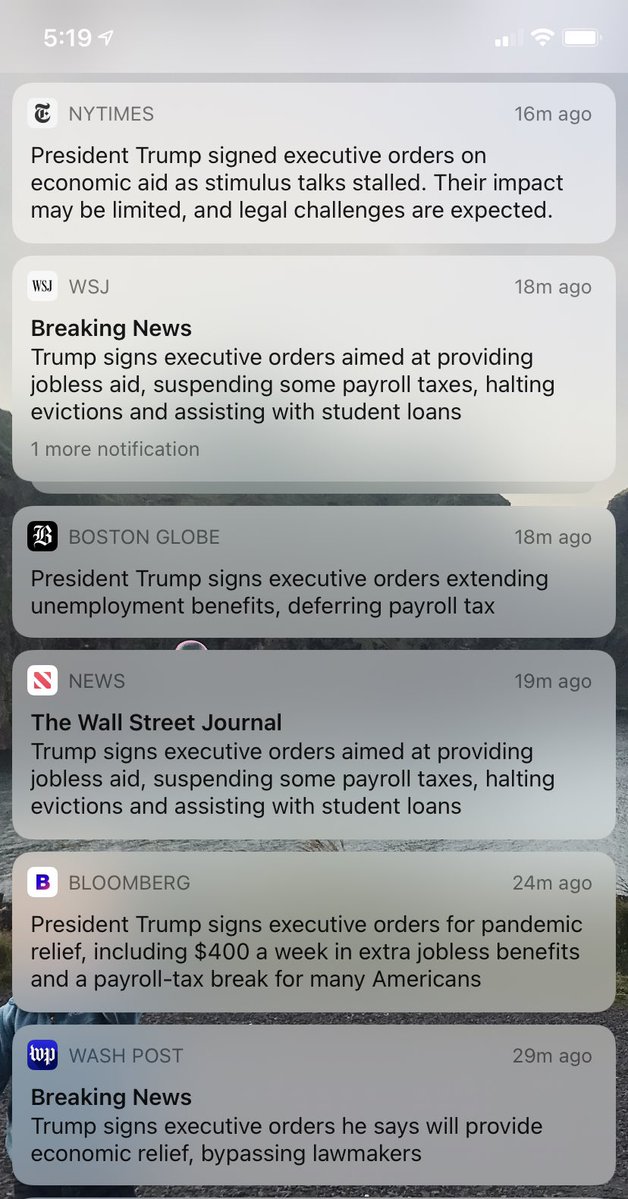
In reality, what Trump signed was a head fake which did jack shit to address problems. Major media failed to portray it that way. To its credit, the Washington Post did sketch this as an end run around Congress — but it was far worse than that.
~ ~ ~
Let’s check with Bharat Ramamurti, member of Congressional Oversight Commission who spelled out the problems in a Twitter thread:
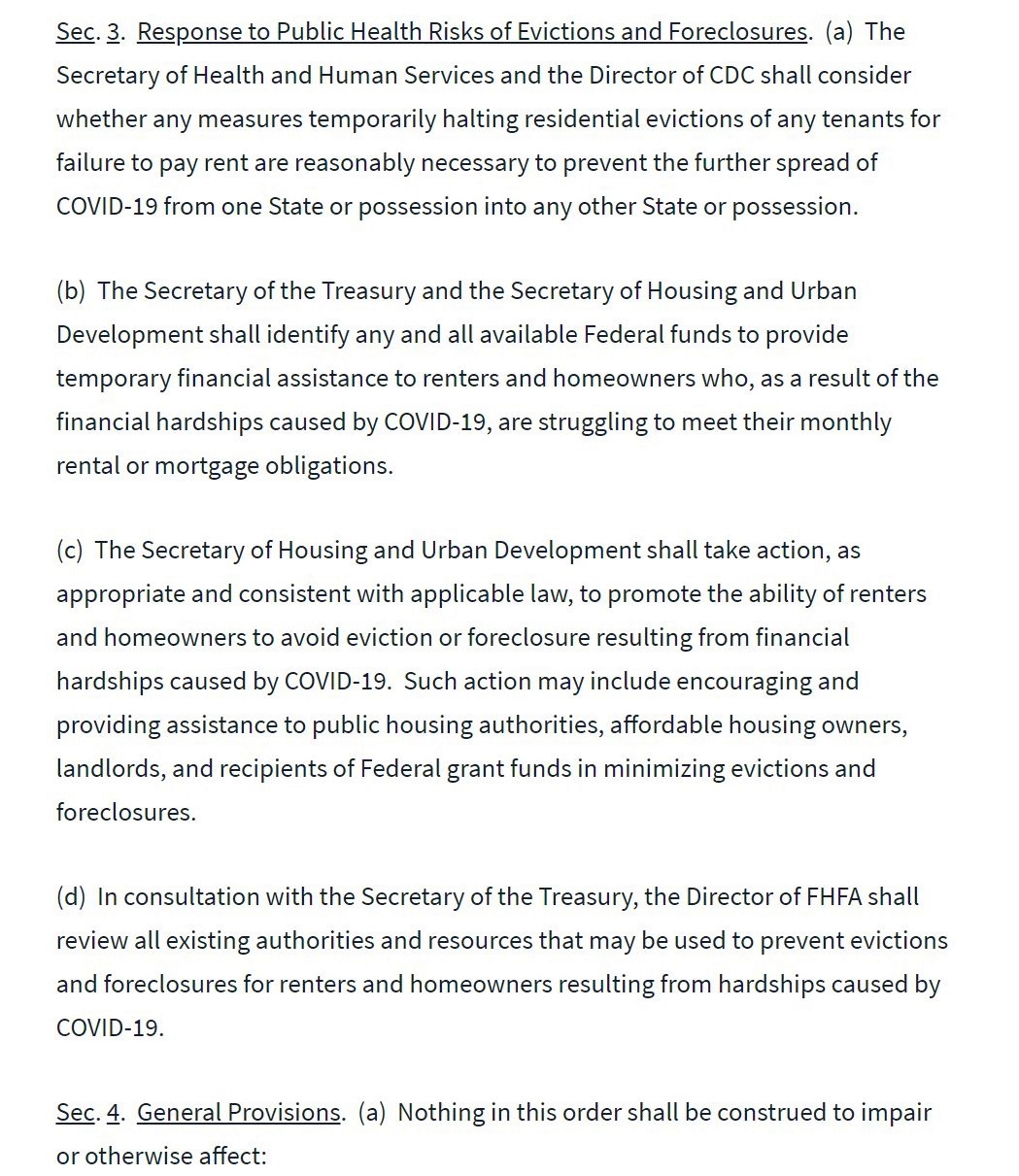
Let’s take a look at the actual text of these executive orders.
Here’s the heart of the one on evictions. As you can see, it doesn’t create an eviction moratorium. It asks certain federal agencies to see if they can maybe do something on evictions.
.
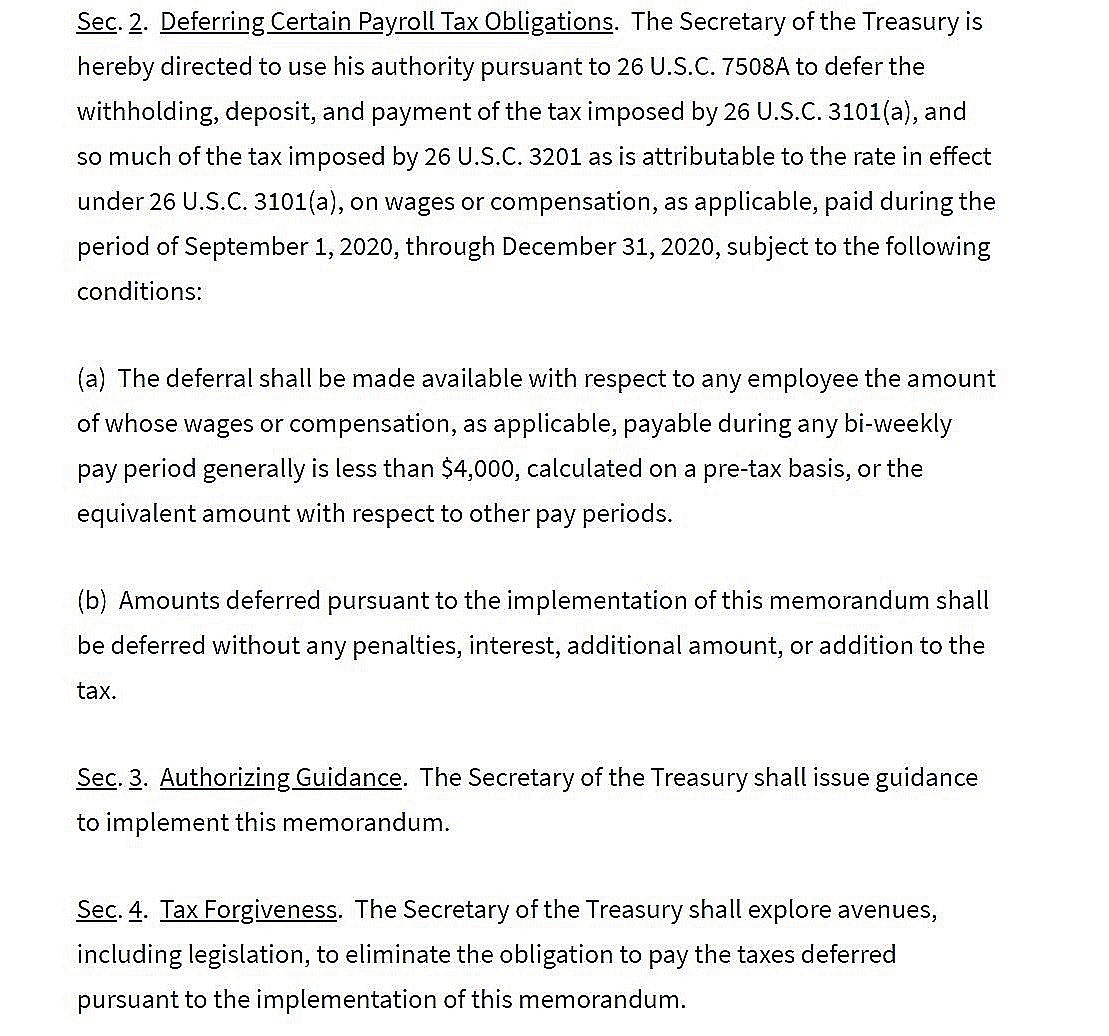
Here’s the payroll tax one. It’s a deferral. That means either employers will continue to withhold your payroll taxes and you won’t see any difference, or they won’t withhold (unlikely), and you’ll have it all withheld from your paycheck when the deferral expires at year-end.
.
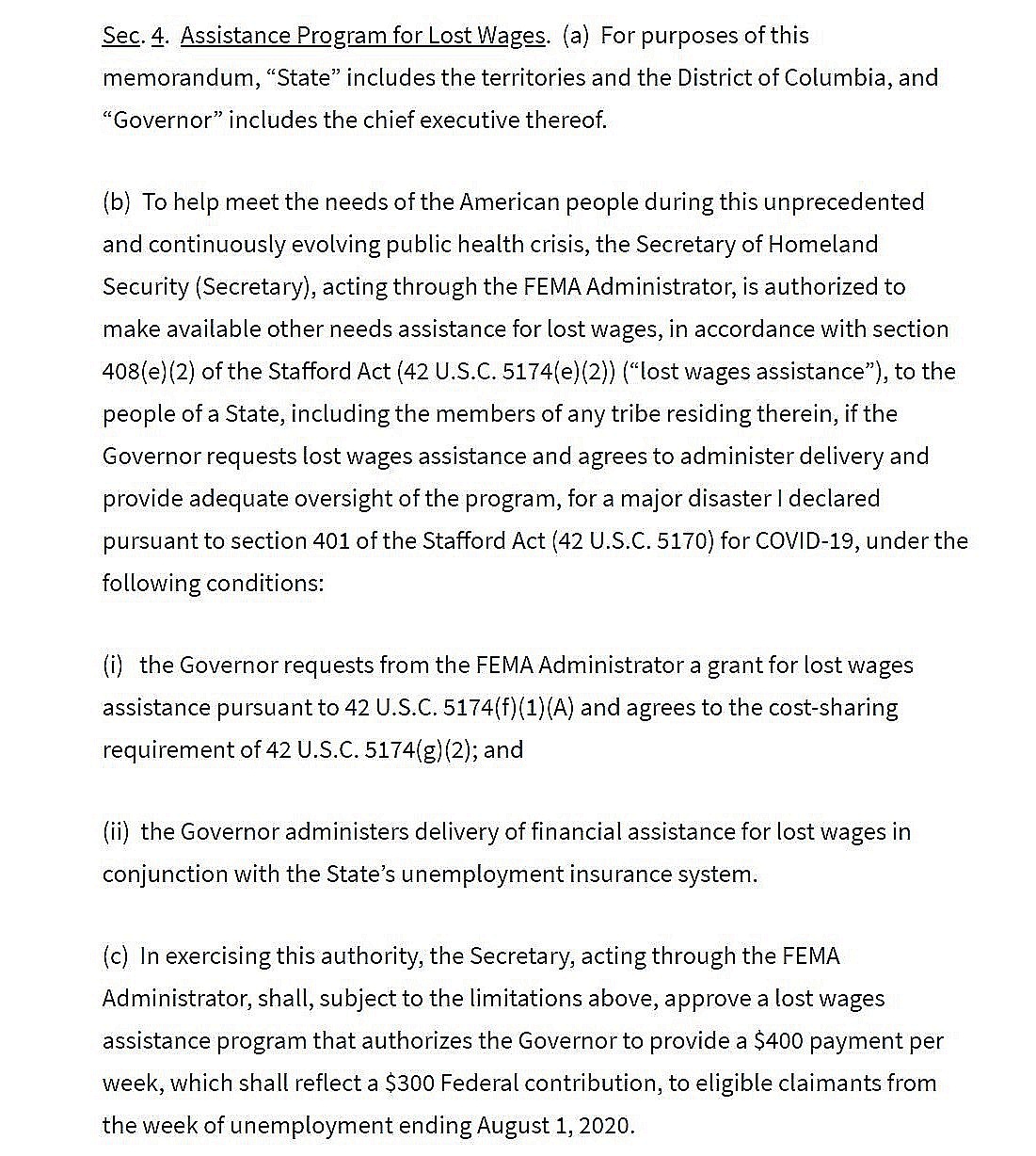
Here is the key part of the unemployment insurance one.
*To be clear, the legal authority to do this is highly dubious.*
But, at best, it’s a $300/week federal contribution redirecting money that, by my estimate, would cover about 4 weeks for the currently unemployed.
.
On unemployment insurance, evictions, and on student loans, these orders and memoranda — even if they are found legal — provide far, far less relief than what Democrats provided in the HEROES Act that passed three months ago and has languished in the Senate ever since.
The House’s HEROES Act passed on May 15. The GOP-led Senate dragged its feet for two months; HEALS Act wasn’t introduced until July 27, offering only a third of the aid the HEROES Act offers while it also contains pork like spending on the F-35.
Because the GOP senate continues to take marching orders from the White House, adhering to an arbitrary $1 trillion limit which is inadequate to the size of the crisis, they avoid good faith negotiation with the House to reconcile the differences between the HEROES Act and HEALS Act.
The White House then throws out useless memoranda to keep the media occupied — a classic Bannon-esque move, treating the media as the enemy by flooding the zone with shit they have proven incapable to process correctly.
The intent is to do nothing. Absolutely nothing.
There is almost nothing actionable in the scribbles: orders like “shall identify,” “shall consider,” “shall take action,” “shall review” are worthless because they are not specific and not supported by legislation which would make them specific.
Nothing in any of the bullshit Trump signed in a reality TV-like gesture will help the millions of Americans already under threat of eviction, or those already evicted like that poor COVID-19 patient in Tennessee.
~ ~ ~
There are a number of analyses already published across the internet which spell out the flaws with the White House’s approach including its fundamental illegality.
Bob Greenstein at the Center on Budget points out the shortcomings in Trump’s “executive actions,” which is a more accurate description than executive orders. What’s missing:
– Funding for testing, contract tracing and other critical publc health needs to help get the pandemic under control
– Food assistance for millions who aren’t getting enough to eat, including students missing out on school breakfast and lunch
– Extension of the federal eviction ban and funding to help renters struggling to pay the rent
– Funding for schools to provide distance learning and take needed precautions to reopen safely
– Funding to keep child care providers afloat so they can care for children safely when parents are able to work
– Fiscal relief for states, including additional Medicaid funding, to avoid more layoffs and cuts in health care and other critical state services
– Employment benefits at adequate levels that would last more than the next six weeks or so for people who have lost jobs.
All the kinds of aid which legislation can provide and an executive order can’t, since the power of the purse lies solely with Congress.
It wouldn’t hurt at this point to brush up on executive orders; the Congressional Research Service worked up a paper on them in 2014. Probably wouldn’t hurt to revisit Youngstown Sheet & Tube Co. v. Sawyer.
As important as wrestling with this executive bullshit is, it’s essential to recognize the White House is absolutely useless to the American public right now. They aren’t doing anything to help the people, only to save their asses in the general election.
A Washington Post article published last evening tells us how chief of staff Mark Meadows and his minions are addressing the pandemic:
As the White House chief of staff, Mark Meadows is responsible for coordinating the vast executive branch, including its coronavirus response. But in closed-door meetings, he has revealed his skepticism of the two physicians guiding the anti-pandemic effort, Deborah Birx and Anthony S. Fauci, routinely questioning their expertise, according to senior administration officials and other people briefed on the internal discussions.
Meadows no longer holds a daily 8 a.m. meeting that includes health professionals to discuss the raging pandemic. Instead, aides said, he huddles in the mornings with a half-dozen politically oriented aides — and when the virus comes up, their focus is more on how to convince the public that President Trump has the crisis under control, rather than on methodically planning ways to contain it.
That’s what they are doing with the economic aid, the same damned thing — head fakes to appease their base, pretending to do something constructive when they’re doing nothing but campaigning.
The White House isn’t interested in addressing the pandemic’s economic problems any more than they are interested in addressing the pandemic itself.
That’s why the pretense of doing anything with worthless executive orders — it only needs to snow the media with head games and prop up Trump until the next head fake is required.
Meanwhile, the country continues to burn out of control.