CDC Modeling Demonstrates Importance of Intervention in Ebola Outbreak

Helpful graphic from WHO illustrating precautions to prevent infection while traveling. Click on image to see a larger version.
As the Ebola outbreak in West Africa continues to grow, fresh attention was focused on it yesterday when the CDC announced that in a mathematical model they developed of the outbreak, failing to intervene in spread of the virus could lead to as many as 1.4 million people infected by late January. Somewhat lost in the response to the “wow factor” of a projection of over a million people being infected is that the model also very powerfully demonstrates how the viral outbreak can be contained simply through moderate adoption of the most basic aspects of an infection control program.
First, to review from my previous Ebola post, Ebola is only transmitted when bodily fluids of infected or dead individuals come into contact with broken skin or mucous membranes.
The key to preventing spread of the virus is for those who care for infected patients, whether they are health care workers at a hospital or family members in the home, is preventing contact with fluids from the patient. CDC has prepared an informative guidance document for how health care workers can control the spread of Ebola in their facilities. The key steps are to provide protective clothing to cleaning staff, use an effective disinfectant, avoid re-use of materials with pourous surfaces and dispose (as regulated medical waste) of all textiles, linens, pillows and mattresses that may be contaminated.
Because practices such as these are routinely implemented in US health facilities when patients with high risk infectious diseases are being treated, there is little to no chance of Ebola spreading within the US. As noted in the previous Ebola post, the extreme poverty of the health care systems in the affected countries in Africa is what has allowed the disease to spread, as health care facilities there simply cannot afford the materials they need for implementing safe practices.
Here is the output of the model for Ebola spread in Liberia and Sierra Leone if infection control is not implemented beyond the current level. As noted in the NYTimes article linked above, the current estimate is that 18% of patients in Liberia and 40% of patients in Sierra Leone are treated in facilities that prevent spread of the virus. The model predicts both the number of infected patients in the two countries and the number of beds devoted to care of those patients (“corrected” means that the estimate for number of infected individuals is corrected for the assumption that 2.5 times more patients are infected than have been officially reported):
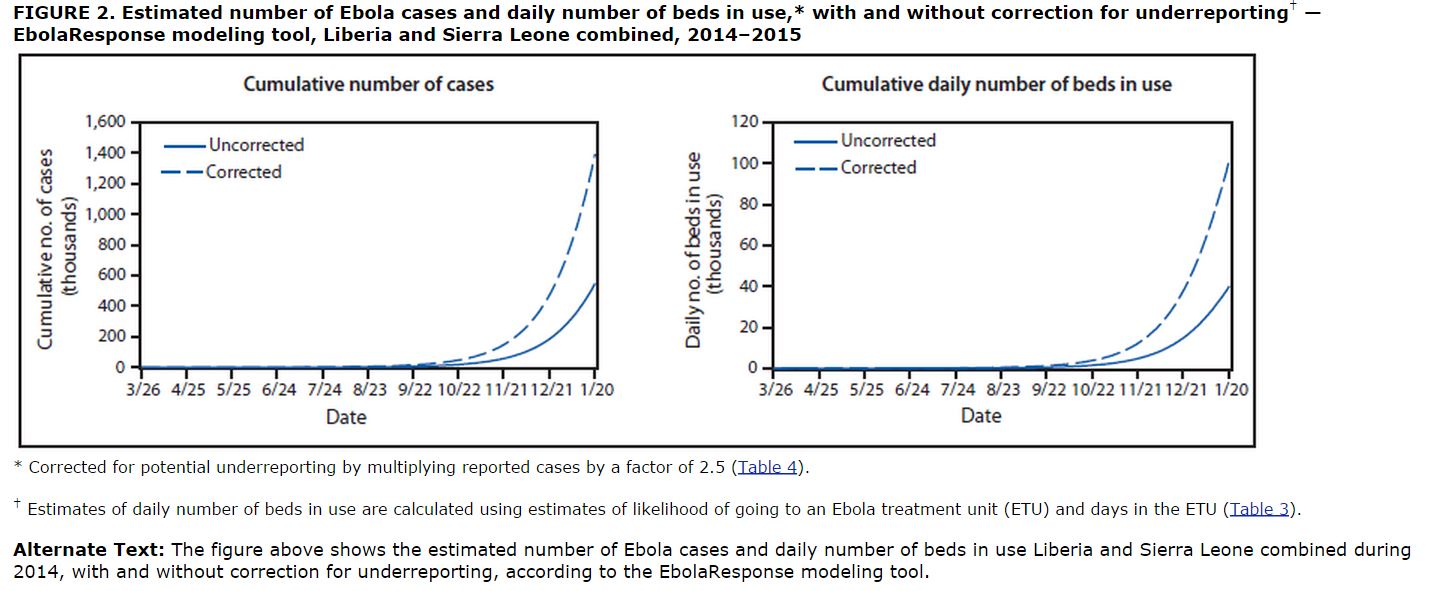
As noted above and widely cited in the press yesterday, if the virus outbreak is left unchecked, the model predicts a cumulative total 1.4 million infected patients in the two countries by January 20 (many of whom are dead by then) and a need for up to 100,000 beds for treatment of these patients.
The good news that is buried in the CDC model is that stopping the virus outbreak does not require implementation of virus control measures for treatment of every infected patient. In the graphs below, we see the output from the model under the assumption that viral control practices start to be implemented now and expand to a level of 70% of infected patients (25% of them in hospitals and 45% in home treatment) being treated under safe practices by December:
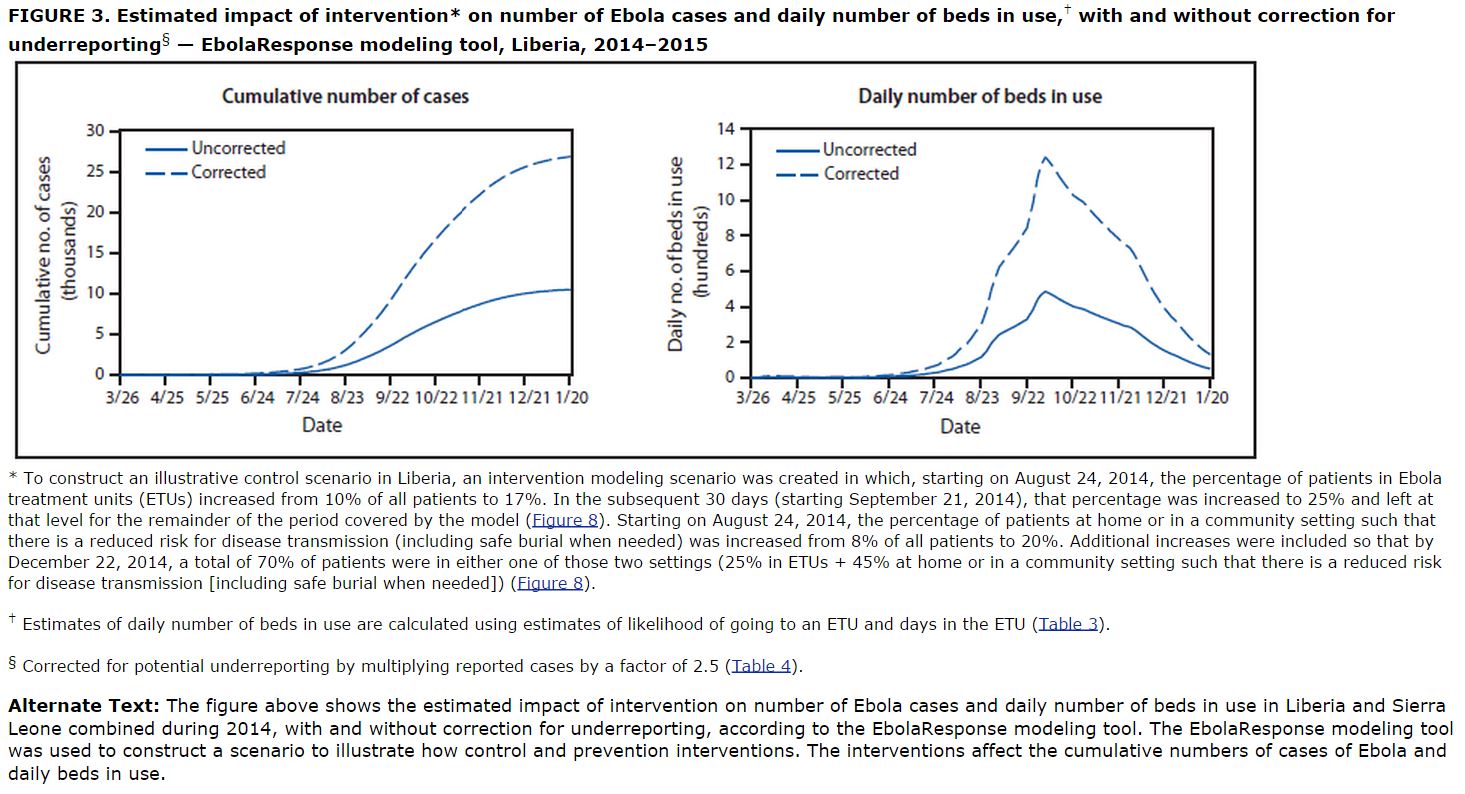
Note that the cumulative number of cases levels off between 25,000 and 30,000 and the total number of beds needed peaks at around 13,000 1300 before dropping rapidly.
This model demonstrates very clearly that the highest priority for stopping the Ebola outbreak should be rapid and widespread implementation of basic infection control practices. Spreading this information into homes where patients are being treated is key. Convincing families of the importance of removing infected clothing and bedding seems likely to be the pivotal aspect of the public information campaign. Help from the West will be essential in providing the huge amount of disposable protective clothing and the necessary cleaning and disinfecting supplies. Replacement clothing, linens, mattresses and pillows should be provided as many of the affected families will be hard-pressed to replace these items under the already difficult conditions of an infected family member.
Further good news is that these projections were based on conditions in August and there is reason to believe that the situation may already be getting better. From the Times, again:
The caseload projections are based on data from August, but Dr. Thomas R. Frieden, the C.D.C. director, said the situation appeared to have improved since then because more aid had begun to reach the region.
“My gut feeling is, the actions we’re taking now are going to make that worst-case scenario not come to pass,” Dr. Frieden said in a telephone interview. “But it’s important to understand that it could happen.”
Let’s hope that Dr. Frieden is correct.
