10 Years of emptywheel: Jim’s Dimestore
As you saw in Marcy’s posts yesterday, emptywheel is celebrating the ten year anniversary of the move from The Next Hurrah to Firedoglake. You will notice that the current version of the blog comes to you without ads. If you want this wonderful state of affairs to continue, contributions are a must. A new subscription option helps to make sure the hamsters keep turning the wheels on the magic blog-hosting machines and the ever more sophisticated mole-whacking machinery stays up to date.
Marcy’s outstanding work over the years has received great acclaim. A huge part of the success of the blog, though, has been its ongoing tradition of the best commenting community on the internet. Over the years, the conversations that have taken place on each seminal post have helped to decipher the meaning of cryptic government documents, bring in alternate views and point out new information as it breaks. In the end, emptywheel isn’t just a blog, it’s a community. For all of your support and participation during these trying times, we thank you.
In keeping with the “10” theme, Marcy has a post highlighting her favorite surveillance posts over each of the last ten years. She has graciously allowed a few of us hangers-on to participate with posts of our own. I haven’t been an official emptywheeler for all of those ten years. I did spend a year as an evening editor at Firedoglake around the time of the migration from TNH, so I got to start my friendship with this group of writers and commenters around that time. I’m going to list my favorite ten posts from the time I started posting here, shortly after the blog moved from Firedoglake to the independent site. Several of these posts link back to earlier work at MyFDL. Sadly, the archives of that work were imperfectly migrated to the Shadowproof successor to Firedoglake, and so searching for those is imperfect and many of the graphics are lost.
So here is Jim’s Dimestore listing my 10 favorite posts on Emptywheel.net, in chronological order:
DETAILS OF SILICON-TIN CHEMISTRY OF ANTHRAX ATTACK SPORES PUBLISHED; WILLMAN TUT-TUTS
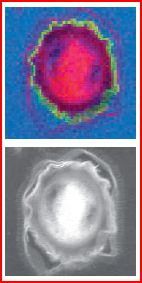
Sandia National Laboratories image of attack spore. In the upper frame, silicon, in green, is found exclusively on the spore coat and not on the exosporium (outer pink border).
Perhaps my favorite topic over the years has been a technical analysis of the evidence presented by the FBI in its Amerithrax investigation. It is absolutely clear from this analysis of the anthrax attacks of 2001 that the FBI failed to demonstrate how Bruce Ivins could have carried out the attacks on his own. This post goes deep into the technical weeds of how the spores in the attack material were treated so that they would disperse easily and seem to float on air. The bottom line is that high amounts of silicon are found inside these spores. The silicon could not have gotten there naturally, and it took very sophisticated chemistry to get it there and treat it to make sure it stayed. Ivins had neither the expertise nor the equipment to achieve this highly advanced bioweaponization. Earlier work I did in this series showed that Ivins also could not have grown the anthrax used in the attacks. My favorite candidate for where it was produced is an isolated lab built by the Defense Threat Reduction Agency on what is now called the Nevada National Security Site (formerly the Nevada Test Site) that Judy Miller described on September 4, 2001. That article by Miller has always stood out to me as the ultimate limited hangout presented by DoD before the fact, where we see a facility of the perfect size for producing the amount of material used in the anthrax attacks. Those attacks occurred just a short time after the article was published. Miller’s assurance in the article that the site only was used for production of harmless bacteria sharing some characteristics with anthrax just never smelled right to me.
INTELLIGENCE AIDE FLYNN RE MCCHRYSTAL: “EVERYONE HAS A DARK SIDE”
When Michael Hastings’ article in Rolling Stone led to Stanley McChrystal’s firing, little did we know that this would be the beginning of the fall from grace for David Petraeus and his all-star band of torture enablers. These “operators”, as Hastings termed the team, relied on night raids and illegal detentions as the core of their counterterrorism initiatives in Iraq and Afghanistan. These foolishly evil practices fueled massive growth in the insurgencies in response. In this post, Flynn reveals to us that he felt McChrystal, and everyone else, has a “dark side”. As we now await fallout from Flynn’s guilty plea for his lies to the FBI about conversations with Russian Ambassador Kislyak (mainly, his testimony against the rest of Trump’s team), it appears that Flynn himself found the dark side to be quite compelling.
DESPITE METAPHYSICAL IMPOSSIBILITY, US GOVERNMENT REPEATEDLY ATTEMPTS RETROACTIVE CLASSIFICATION
Another favorite topic of mine over the years has been the utter futility of the military’s efforts to “train” troops in both Iraq and Afghanistan. It has been an endless sequence of the military getting countless “do-overs”, with Congress rolling over and believing every single utterance of “This time it will work for sure!”. Part of the military’s strategy in hiding their training failures was to keep changing how Afghan troops were counted and evaluated for combat readiness. A corollary to the futility of the training effort is the horrific death toll of “green on blue” attacks, where the Afghan or Iraqi trainees attacked and often killed those who were training them. When this problem got especially bad in Afghanistan in 2011, DoD commissioned a sociological analysis that returned a result the military did not like. The report indicated that the military was utterly failing to address vast cultural differences between Afghan and coalition troops. The military, in its infinite wisdom, decided to classify the report, but did so after it already had been released in unclassified form. Oops.
PERSIANS PUNK PHOTO PRETENDERS: PARCHIN PRETTY IN PINK

Detail from the photo carried in CNN’s story showing the pink tarp over the building said to contain the blast chamber.
Neocons have long lusted after violent regime change in Iran. Cooked up allegations on Iran’s nuclear capabilities have played a central role over the years in how they wished to achieve that war. Despite the neocons’ best efforts to sabotage negotiations, Iran agreed to a comprehensive set of severe restrictions on its nuclear capabilities in return for “dropping” (quotes because the US has claimed other grounds for maintaining other sanctions) the worst of the US sanctions that crippled Iran’s economy. Along the way, I had a ton of fun picking at two of the worst offenders in spreading anti-Iran propaganda: David Albright of the Institute for Science and International Security and George Jahn of AP. Reports that Iran had constructed a high explosives blast chamber at the Parchin military site became quite a point of argument. Albright spent countless hours scouring satellite images of the site and claimed the photographs showed that Iran was attempting to clean radioactivity from the site. Iran seemed to have a lot of fun with this process. I’m sure the pink tarps in the post here were added just to punk Albright. I maintained that the real evidence of what had taken place at the site couldn’t be scrubbed, because the accused activity would have resulted in the steel chamber itself being made radioactive throughout its entire thickness. Perhaps Iran made the same assessment, because once the IAEA gained access to the site, there was no steel chamber to be found. Was there ever a blast chamber there? Who knows? In the end, whether Iran carried out that work is immaterial, as the Joint Comprehensive Plan of Action has the most aggressive inspection regime ever agreed to by a country that hasn’t just lost a war. We can rest assured that Iran has no capability at the current time of assembling a nuclear weapon, and the neocons are left to pout about diplomacy working better than their war ever could have. If you want to know why Donald Trump put Rex Tillerson in charge of dismantling the Department of State, look no further than the success diplomacy played in achieving the JCPOA.
JOHN GALT KILLS TEXANS IN MASSIVE FERTILIZER PLANT EXPLOSION
When a massive explosion in West, Texas killed 15 people, injured over 250 and destroyed 500 homes, it was clear to me who had killed these Texans: Ayn Rand’s mythical libertarian hero John Galt. How else do you explain a site being allowed to store hundreds of thousands of pounds of ammonium nitrate with inadequate fire protection and fatally close to inhabited structures than the misguided libertarian belief that free enterprise should rule? In the post, I pointed to the dangers inherent in the lack of zoning laws that allowed this fatal mixture of structures. As we later learned from the Washington Post, John Galt’s influence on the destruction was decades in the making:
The plant was a mom-and-pop operation, a distribution center where farmers picked up custom mixes of fertilizer to boost crop yields. It was built in 1962 a half-mile outside West. As the harvests grew, so did the town. In 1967, the rest home opened 629 feet from the plant. In the early ’70s, a two-story apartment complex was built even closer. Then a playground and basketball court, a mere 249 feet away.
We learned last year that ATF has determined that the fire that preceded the blast was intentional. So while we don’t know who started the fire itself, we know for a fact that, ultimately, it was John Galt who killed these 15 Texans.
US DRONE STRIKE IN PAKISTAN REEKS OF POLITICAL RETALIATION YET AGAIN
The current concern that Donald Trump will lash out in fury with a nuclear strike, somewhere, anywhere, just to vent his anger over Mueller’s noose tightening over his entire administration is not the first time that it was appropriate to be concerned about an enraged high-ranking government official killing innocent people. In the case of John Brennan, poorly targeted rage attacks carried out as retaliation for a perceived wrong happened repeatedly. In the post linked here, a drone strike in Pakistan’s tribal area seemed timed as retaliation for Pakistan refusing to reopen supply routes that had been closed six months earlier when the US killed 24 Pakistani troops in an erroneous attack. The post goes on to detail other rage drone strikes that Brennan ordered, with the worst probably being the killing of over 40 people who were simply gathered to discuss mineral rights. That strike was carried out the day after the CIA’s Raymond Davis was finally released and was clearly carried out without proper evaluation of targeting criteria, as it seems few if any actual terrorists were killed.
NO, WE AREN’T ALL GOING TO DIE BECAUSE EBOLA PATIENTS ARE COMING TO US FOR TREATMENT

Scary, color-enhanced electron micrograph of Ebola virus particles. Creative Commons license courtesy of Thomas W. Geisbert, Boston University School of Medicine.
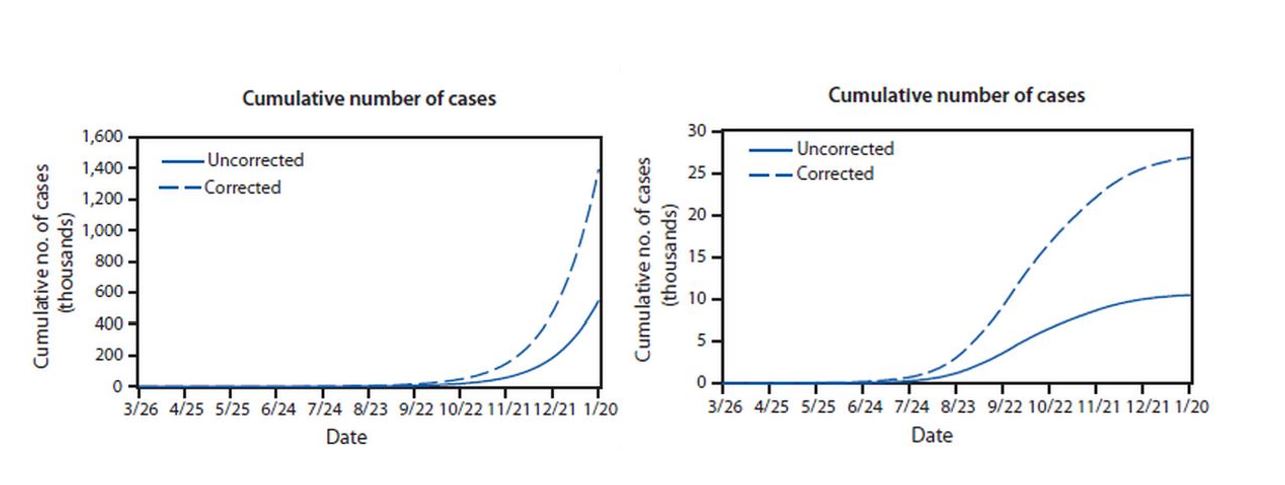
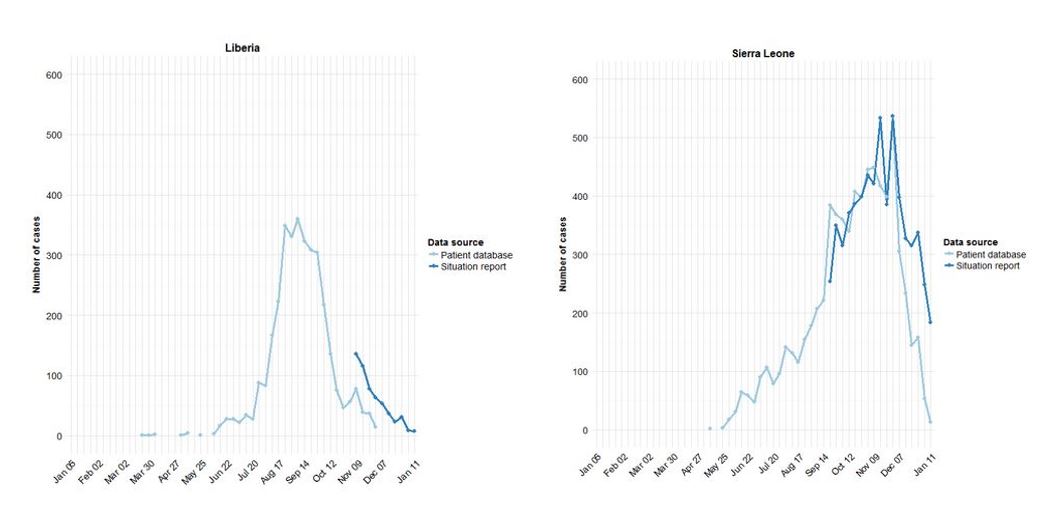
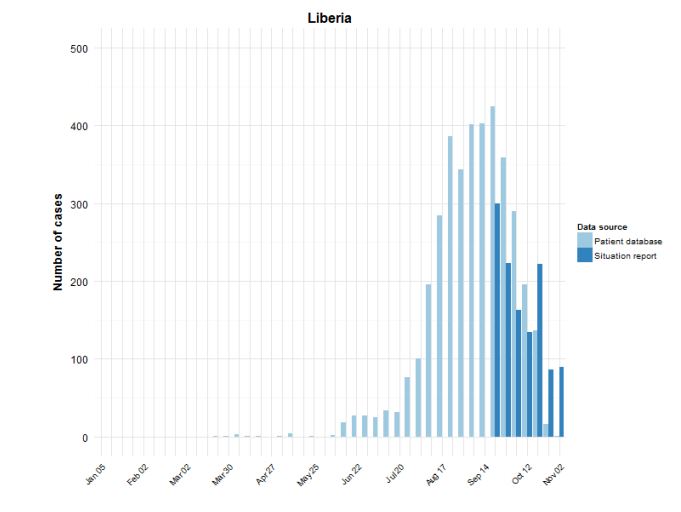
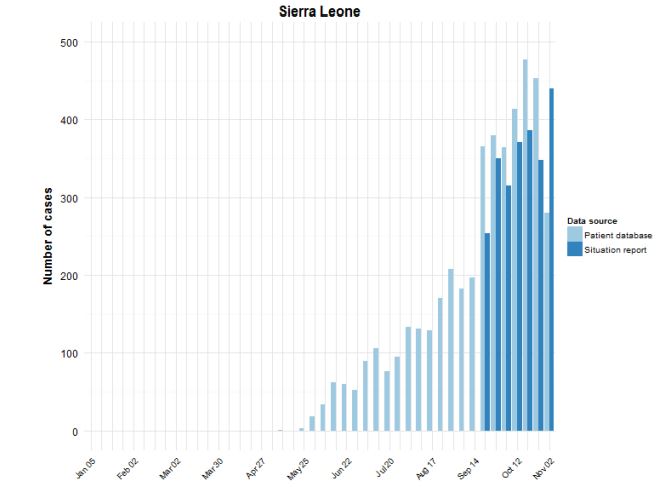
The Ebola outbreak in 2014 led to widespread fear in the US, especially when it was announced that medical personnel who had been treating Ebola patients in Africa and became infected would be transported to Atlanta for treatment. There was no appreciation for how the disease actually is spread, what the conditions were where the medical workers became infected in Africa and how such spread would be much less likely in a properly run US hospital. A poorly run hospital in Texas, however, did manage to have personnel treating Ebola acquire infections. Of course, the treatment at CDC in Atlanta was carried out without incident, and the virus did not spread in the US, even after the Texas hospital had its initial failure. In fact, as the virus wound down, those who study and understand the virus were shown to have been completely correct in their analysis when they modeled how large the outbreak would get before receding once proper intervention was carried out. But the fears of Ebola wiping out the US weren’t the only bit of bad science that had to be knocked down during the outbreak. Conspiracy theories started spreading that the Ebola virus in the 2014 outbreak had been genetically engineered in a bioweapons lab and was accidentally released from a lab in Africa. DNA sequence analysis quickly debunked that one.
WASHINGTON POST FAILS TO DISCLOSE HEINONEN’S UANI CONNECTION IN ANTI-IRAN OP/ED
Yes, the Iran nuclear agreement is so important that it is the only topic repeated in my ten favorite posts. In this post, we are in the time just a few months before the agreement is finalized, and the neocon opponents of the deal are reaching a fever pitch. The post outlines a horrible failure of full disclosure by the Washington Post. This occurred after Bezos purchased the paper, but clearly was a failure of beating back the darkness in which democracy dies. In this case, the Post carried an op-ed opposing the Iran deal. Besides allowing an incendiary headline (The Iran Time Bomb) and giving voice to Michael Hayden and neocon nightmare Ray Takeyh, the Post made its biggest failure regarding the middle author, Olli Heinonen. The Post allowed Heinonen to identify himself only by his current Harvard affiliation and his former role in IAEA. What is left out of that description is that Heinonen was also playing a prominent role on the Advisory Board of United Against Nuclear Iran, shadowy group with even more shadowy funding sources. Somehow, in the course of its “advocacy” work against Iran, UANI had come into possession of US state secrets that suddenly allowed it to avoid a civil case for defamation of a businessman they accused of breaking sanctions against Iran. Why, yes, of course the New York Times also allowed Heinonen to deceptively carry out his work on their pages, too. This time it was in a “news” story that came out shortly after the UANI civil court case was dismissed when the judge stated the case could not proceed because of the state secrets involved. Of course, even after more than two and a half years, neither the Washington Post nor New York Times have admitted their omissions in describing Heinonen’s affiliations in the cited articles. It is really remarkable that diplomacy defeated this full court press by the neocons who were working with the full cooperation of the media.
WAVING THE CONSTITUTION AT THOSE WHO IGNORE IT
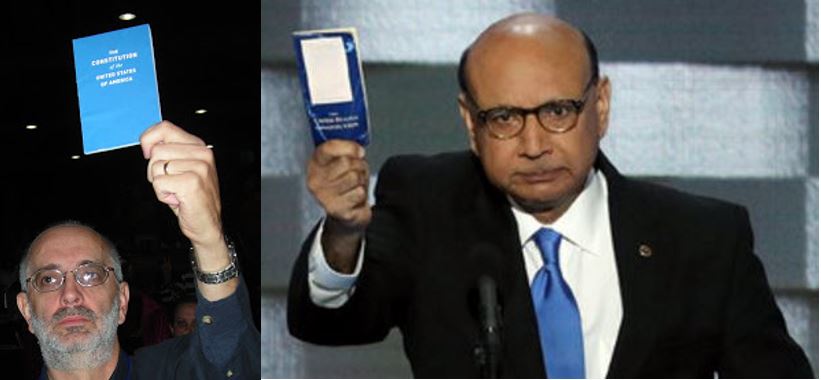
I waved my pocket copy of the Constitution at Nancy Pelosi on July 19,2008. Khizr Khan waved his at Donald Trump on July 28,2016.
I haven’t written much in the last couple of years, but I just couldn’t avoid writing this one only ten days after surgery to replace my aorta. When I saw Khizr Khan’s appearance at the Democratic National Convention, I was really moved when he waved his pocket copy of the Constiution at Donald Trump. I had done the same thing in July of 2008 when Nancy Pelosi appeared at Netroots Nation in Austin. I was waving my Constitution at Pelosi to remind her of her failure to impeach George W. Bush and Dick Cheney for their roles in torture and illegal wars. Khan was calling out Trump for his campaign promises that so clearly violate the Constiution. Sadly, Trump has followed through in enforcing many of those policies Khan warned us about and we are left without much more recourse than continuing to wave our Constitutions at those who violate it on a daily basis.
ON JULY 2016 PANEL, GEORGE PAPADOPOULOS USED SAME COVER ORGANIZATION AS JOSEPH MIFSUD
My one minor contribution so far to the unfolding saga of Russian influence on the 2016 election was prompted by noticing a photo in my Twitter stream shortly after the George Papadopoulos plea agreement was made public. What initially caught my eye was that my Congressman, Ted Yoho, was in the photo with Papadopoulos while both appeared in a panel discussion in Cleveland in July of 2016. However, once I started digging into the circumstances of the photo, I discovered that when he appeared for the panel, Papadopoulos claimed an affiliation with an entity that was also an affiliation for the shadowy Joseph Mifsud. We still don’t have a satisfactory explanation of how these two came to have a shared cover organization where it seems both Papadopoulos and Mifsud had positions that were grossly inflated with respect to their previous career accomplishments. I still think that if we ever discover who was behind these two getting such inflated positions, we will learn much about who might have been orchestrating later events in which these two played roles.