This Is My O Face: Welcome, Omicron [UPDATE-1]
[NB: check the byline, thanks. Scroll down for update and new content. /~Rayne]
Well, it had to happen sooner or later given this pandemic’s craptacular start and the inability of Trumpy right-wingers, nation-states with fewer resources, and Global Big Pharma to tackle COVID’s spread.
I’ve got what feels like a chest cold – gravelly upper chest, scratchy throat – and my spouse has the scratchy throat.
I’ve been around exactly five people in the last two weeks, one of which is my spouse; the others are my kids and two friends. All of them are fully vaccinated and boosted as are we two in my household.
Their status doesn’t rule out the possibility that one of them may carried the virus, if indeed we’re infected. Vaccinated folks can carry the virus.
No lost of smell or taste noted. No other symptoms so far. In my case this might not even be COVID; with the crazy windstorms we’ve had this week I’ve inhaled a bunch of dust every time I’ve had to go outside which may have triggered a flare of my autoimmune disorder.
But if Omicron results in milder symptoms especially in fully vaccinated persons, I may well have COVID.
Put me down as Status: Pending until I’m tested and receive my results.
There will be more to this post when I get back from the testing center, watch for an update.
~ ~ ~
UPDATE — Saturday 18-DEC-2021 -–
That’s not how I intended to start a post about the Omicron variant, but here we are: we go with the virus we have, not the one we wish we had.
What we know about Omicron so far is still rather loose and ill defined. Part of the challenge is that Omicron meets a different population than Alpha or Beta did last year – depending on the country there’s such a broad mix of people who are partially vaccinated, fully vaccinated, boosted, and with different mixtures of vaccinations as well as the stubbornly unvaccinated and the previously infected who occur in each category along with the immunocompromised.
When the first wave hit, everyone everywhere was unvaccinated. There was no need to sort the population except for those who may have been previously infected. By the Delta-dominant third wave analysis was slightly more complicated as more people were vaccinated or previously infected.
Now there’s so much more to sort through to identify trends. I wouldn’t be surprised if there are still surprises in case data as Omicron infections explode.
And explode they will, doubling every three days — if not more in less time.
I still can’t wrap my head around the number of cases this variant is expected to produce. I’d like to recommend you listen to this Twitter Spaces recording of a discussion with Financial Times’ statistics journalist John Burn Murdoch, pharma correspondents Hanna Kuchler, Jamie Smyth, and Donato Mancini, and senior editor Clive Cookson.
Link: https://twitter.com/FinancialTimes/status/1471134080175689731
A caveat before you dive in: the discussion has a UK+EU bias given the location of the participants and their employer. The UK’s handling of COVID has been absolutely abysmal to date and may shape their perspectives.
An even bigger caveat: Twitter Spaces self-delete in 30 days, so you only have 27 more days to listen to their discussion. Catch it before January 13, 2022.
I also can’t wrap my head around the dramatically increased contagiousness of Omicron versus Delta. Delta was already much more contagious than the initial dominant variant; its electrostatic charge caused the aerosolized virus to be attracted to soft human tissues like magnets.
Omicron, though, is 70 times more infectious† than Delta. Just fucking mind boggling, this jump from Delta, and what it means for this winter as we approach the holidays.
A preliminary study suggests the Omicron variant is better at transmission because it infects the upper airway, but bad at infecting the lower lungs explaining why it presents with milder symptoms than its predecessor, Delta. Attaching itself to tissues higher in the airway the virus can be more easily dispersed in aerosol, but lower in the lungs the virus is more difficult to blow out.
The increase in infectiousness† means you MUST upgrade your masks, especially before holiday gatherings in enclosed spaces. Fabric alone will no longer do the job even if everyone in the same shared space is wearing them. This goes for health care workers, too, who’ve continued to wear surgical masks through the pandemic when they could get their hands on them. All of us need to be wearing N95 masks in shared public spaces to reduce transmission.
Testing will become more critical because Omicron may present for many like common cold symptoms, hence my scramble yesterday to get tested. A year ago I might have blown off the symptoms I had because I didn’t lose my sense of smell and/or taste, didn’t run a temperature, didn’t have breathing problems or feel like I was losing oxygen. But not now – I can’t do that.
Nor can we ignore the fearsome possibility of co-infection or super-infection as mentioned in Financial Times’ discussion, in which the infected has both Delta and Omicron at the same time. Imagine this kind of scenario creating conditions for development of a new variant which is everything bad about Delta and Omicron combined. There’s also the possibility of co-infection with influenza, which has already happened though infrequently so far.
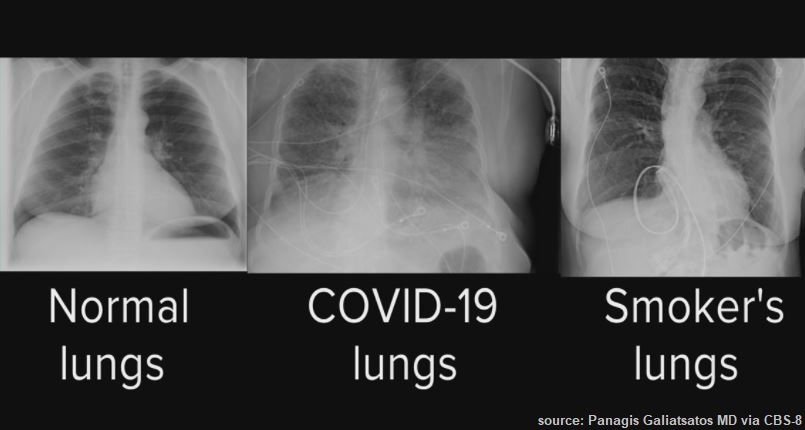
If this is what lungs looked like with the earlier variants, what will they look like with a super-infection of Delta and Omicron combined? Will we see more patients in need of lung transplants even earlier? Will we simply see an increase in mortality?
Only time, observation, and data will tell, and we’d really rather not accrue any data.
One thing we have learned about Omicron: the Johnson & Johnson adenovirus-vector one-shot vaccine is not effective against it, based on a study (pre-print) by Vir Biotechnology Inc. employees published this past Wednesday.
Electric light bulbNew VACCINE RANKING of ability to neutralize #Omicron—Moderna appears to be the strongest against Omicron in this study, but still big drop. Pfizer next best (but we know infection efficacy is 30-34%), AstraZeneca & Sinopharm poor. J&J & Sputnik = zero.Thread https://t.co/5xmnXH2XaJ
3:33 AM · Dec 15, 2021·Twitter for iPhone
The Center for Disease Control issued a statement of preference for mRNA vaccines as well given the risk of death from unusual clotting observed across the population vaccinated with J&J. This means if you are J&J vaccinated but unboosted, you should look into an mRNA booster as soon as possible. This is fluid and may be subject to change; I wouldn’t be surprised with Omicron’s explosion of cases to see revaccination with a full regimen of mRNA recommended for J&J recipients.
~ ~ ~
Besides this unexpected Chinese fire drill of chasing COVID tests and results, what’s really frustrating is the continued absurd nihilistic conservatism of many unvaccinated and their maskless counterparts.
Exhibit A: Matthew Walter, arch Catholic, editor of The Lamp, contributor to the American Conservative, and the author of “Where I Live, No One Cares About COVID,” unfortunately published by The Atlantic.
Let’s make a distinction here between the folks who are still struggling to get vaccinated because of vampiric capitalism and racism. Many unvaccinated people want to be protected but can’t take the time away from work to get their shots and deal with the possible symptoms which often follow the vaccine. We forget too many Americans living in precarity risk losing their jobs if they or their family members are sick because this country hasn’t ensured a reasonable amount of paid time off for illness let alone health maintenance. These same workers end up gambling on not getting COVID because they can’t afford to take a handful of days for the vaccinations and booster for themselves and their family. If COVID gets them, well, they know it’s all over.
Ditto the unvaccinated who have legitimate health conditions which preclude vaccination. For them the rest of us should be vaccinated.
But the deliberately unvaccinated and COVID indifferent who identify with Matthew Walther? Fuck them.
All those stupid assholes like Walther who’ve decided to pretend there’s no pandemic, choosing instead to party on Michigan’s Torch Lake’s sandbar back in July 2020, causing a superspreader event? Fuck them all, the selfish gits.
Fuck all the jerks fighting mask and vaccine mandates, who’d rather kids and their teachers got sick with COVID, causing more superspreader events.
Sure, I get it – Walther wrote his misbegotten spike-worthy piece for The Atlantic from his deep red rural St. Joseph County located on the Michigan border with red state Indiana. The Atlantic’s editors stupidly decided to both-sides the pandemic.
But The Atlantic failed to look at what side they were giving oxygen by platforming Walther. The town in which Walther’s journal The Lamp is published has a population of less than 8000.
And they’re white, white, white.
It’s a super homogenous location where nobody gives a shit about COVID because nearly 90% of them share the same everything from skin color to politics. They act as if the only people who get COVID, are disabled by it or die from it are those people in Metro Detroit area. That’s the hidden subtext in Walther’s essay.
The Ameri-centric xenophobia also rolls off Walther:
…Indeed, there is something small-minded and puritanical and distinctly American about the whole business of obsessing over whether vaccinated teachers remove their face covering during a long school day. …
Shall we ask Japan and South Korea about mask wearing and other COVID mitigation measures? Japan’s population is 38% of the U.S. and has had less than 19,000 COVID deaths to date, while South Korea at 15% of U.S. population has had less than 5,000 COVID deaths in the same time frame.
Apparently the world doesn’t exist outside predominantly white spaces like the U.S. and Europe for Walther. We look like morons not only because of the ongoing mass death event but because folks like Walther insist there’s nothing to see, move along.
But I, too, live in Michigan, in a limnal space between a suburb and rural Michigan. It’s not just those people who are getting sick, hospitalized, disabled, or dying because of COVID. Here we all know quite a few white people who’ve died of COVID, the disease Walther doesn’t give a shit about any longer; the obituaries scrolling by on the local television stations are wall to wall with these white faces.
It’s not just these disposable people to whom Walther is indifferent who are casualties. COVID is chewing up our health care system capacity to the point the feds have sent in support personnel; it’s eating the spirit of our health care workers to the point where many are leaving health care permanently.
ER doctor Rob Davidson lives and works only four counties and a hundred miles north of Walther, in a community which is even smaller and whiter than Three Rivers:
Don’t miss @DrRobDavidson’s latest conversation with @JoyAnnReid about the difficulty health care workers face seeing patients suffer and even pass away from COVID-19 instead of taking the safe, effective vaccine. https://twitter.com/i/status/1471919814159523840
2:06 PM · Dec 17, 2021·Twitter Web App
If you follow Dr. Davidson on Twitter you know how frustrated he and health care workers are to care for so many who are deathly ill and too often die when the disease could have been mitigated or prevented with a readily available vaccine regimen. Many of the people lost are friends and neighbors who refused to get vaccinated.
As Davidson notes, “…they’ve been poisoned with this idea that A, COVID’s not a big deal from the beginning and B, these vaccines will somehow make them sick.”
That’s what Walther’s piece continues to validate and nurture because it was platformed by The Atlantic – the other Big Lie which Trump began and continues with propping up by right-wing wretches who treat others’ lives like so much toilet paper, supported by media complicity and click-bait cupidity.
When the pandemic began, Trump wanted to save his own ass at the polls so he repeatedly assured his weak-minded base that COVID wasn’t a big deal, it was a hoax, it would disappear.
Except it was American’s lives which disappeared – more than 800,000 so far, of which more than a third could have been saved by vaccines had Trump left a distribution plan in place instead of another Big Lie.
Nearly double that 800,000 have been lost if excess deaths are included due to COVID’s drain on our health infrastructure.
Which means we’ve lost roughly two million Americans because of Trump’s other Big Lie – a passive-aggressive democide by active neglect.
The capper on Walther’s nihilistic crap: while he claims nobody cares about COVID, a couple thousand people are slogging away in Portage, a mere 26 miles north of Walther’s digs.
They’re producing as much of Pfizer-BioNTech’s Comirnaty vaccine as fast as they can. There’s a Pfizer plant under construction to expand production of injectables which will bring 450 more new jobs. Other biotech companies and their workers in southeast Michigan support Pfizer’s production.
These Michigan residents and employers care one hell of a lot about COVID, and they’ve saved millions of lives.
Which makes Walther’s op-ed look like what it is, an extension of Trump’s democidal lie and an insult to the conscientiousness and humanity of fellow Michigan residents.
A literal insult to neighbors who may be commuting from Walther’s town to make life-saving vaccines every day.
I hope some day Walther meets his Catholic god and is told what an offense it has been that he treated other human’s lives with so little respect and dignity.
~ ~ ~
Status update: Both my antigen and PCR tests came back negative. My coughing is subsiding, leaving just the occasional tickle. I hope this was just an extremely mild cold or an autoimmune flare. But I’m now back on heightened alert; if this was a cold, how did I get it? Could I have infected one or more of the few people I’ve been in contact with this week?
Stay safe, peeps. Don’t drop your guard just yet. Get your booster shot, and a flu shot, too.
____
† Commenter “Doug Fir” took exception to the use of the word “transmissibility” and the substitution of the word “infectious.” Reporting across the media ecosphere has used transmission/contagion/infection and variants of these words interchangeably; this is a point needing further explication and explanation by researchers who are still studying Omicron’s differentiation from other variants. I’ll point to this excerpt from an article in StatNews also linked above as the most thorough reporting but still not definitive as it is based on preliminary data:
The new research comes from a Hong Kong University team led by public health professor Michael Chan Chi-wai and pathologist John Nicholls. Previously, the researchers pioneered a method for growing human tissues extracted from the lung and respiratory tract, which they used to study how SARS-CoV-2 invaded cells and replicated compared to other dangerous coronaviruses. Using this same system, they analyzed how live, replicating particles of Omicron infected the tissues. They found that over the first 24 hours, Omicron multiplied about 70 times faster inside respiratory-tract tissue than the Delta variant. When they ran the same experiments with the lung tissue, they found Omicron was actually worse at infecting those cells than either Delta or the original strain of the virus that originated in Wuhan.
That seemingly helps explain the variant’s infectiousness, and also why it may not be causing as severe sickness as previous variants of the coronavirus — as early data suggest.
“That basically tells us it’s inherently more transmissible,” said Müge Çevik, a clinical lecturer in infectious diseases and medical virology at the University of St. Andrews School of Medicine in Scotland. “The reason Omicron is spreading so fast is not just because of immune evasion” — its ability to elude antibodies from vaccines or infection with earlier variants — “but a combination of that with intrinsic enhanced infectiousness.”
It appears Omicron is not as effective as Delta in attaching to tissues deeper in the lungs; it attaches more effectively to the trachea and bronchi or upper airways where it can be more easily blown out as aerosol others can inhale especially if not well masked and in enclosed shared space with poor ventilation.

