[NB: check the byline, thanks. /~Rayne]
I’ve been sick with COVID this past week, missing the first classes of the fall semester.
I was exposed by a cancer patient who finished a second round of chemotherapy earlier this month. They weren’t vaccinated within the last year because they were undergoing chemo.
They were exposed after Saturday evening mass at their Catholic church in Florida, where others around them were likely not vaccinated, and definitely unmasked, unlike the cancer patient. A dementia patient who refused to mask was the vector between the congregation and the cancer patient.
The cancer patient is still recovering and now at about 90% of their capacity. They’re moving very slowly, thinking just as slowly. They can’t be left alone because they don’t have the reaction time they used to have.
I’m about 95% recovered, still have some sinus congestion and lingering crud in my chest. My ribs and my throat feel still feel bruised from hacking up my lungs so hard earlier this week.
What I’m not certain I’ll recover from is the trauma of having to check my father the cancer patient for a pulse last week when he collapsed on the kitchen floor, reviving him, getting him up and moving and into my car so I could rush him from their remote home to an urgent care facility more than 30 minutes away.
I didn’t think to put a mask on him or a mask on myself at the time because I was worried something had gone very wrong after my dad’s two-year fight with cancer. I was worried about the monsoon-like storm I had to drive through to get to urgent care. I thought erroneously he had recovered from COVID and wasn’t contagious because he hadn’t had a fever and he hadn’t been coughing.
So I unintentionally hot boxed my dad’s COVID-laden exhalations in my car for 30 minutes trying to save my father. I’d do it again if it came down to it but I should never have had to.
This country has been deeply damaged enough by the anti-vaccine movement since the COVID pandemic began; it shouldn’t have to face worse.
~ ~ ~
By now you’ve read Peterr’s Thursday post about the government’s internecine warfare at the Centers for Disease Control and the excision of director Susan Monarez, followed by the protest resignations of senior CDC staff in support of Monarez. The senior staff who resigned are:
• Demetre Daskalakis, former director of the National Center for Immunization and Respiratory Diseases
• Debra Houry, former chief medical officer and deputy director for program and science
• Daniel Jernigan, former director of the National Center for Emerging and Zoonotic Infectious Diseases
• Jennifer Layden, former director of office of public health data, science, technology
Each of these individuals has a deep background and education in medicine, healthcare, or public health. None of then should have been expected compromise themselves to support our nation’s public health.
None of them should have been treated so shabbily by RFK Jr.’s shit-tastic management of HHS. It’s not at all hyperbole to call it shit-tastic; I strongly recommend listening to The New York Times’ podcast interview with Demetre Daskalakis because it will rid you of any doubt the label is deserved.
Here’s an excerpt I found particularly telling:
DASKALAKIS: Yeah. So this was not related to ACIP, the announcement by the Secretary to change the childhood schedule. I learned about the change of the childhood schedule on X.
ABRAMS: You learned about it on social media —
DASKALAKIS: Yes, ma’am.
ABRAMS: — like the rest of us.
DASKALAKIS: That is correct.
ABRAMS: Wow.
DASKALAKIS: So I was sitting in a meeting with senior leaders at CDC. And as I was sitting there talking about the outbreaks that I was managing, my phone blew up with, “I didn’t know you guys were changing the children’s schedule.”
ABRAMS: People texting you?
DASKALAKIS: Yeah.
ABRAMS: Wow.
DASKALAKIS: Not from HHS, people in the world. Because they saw —
ABRAMS: People in the world, your friends and family or whoever seeing this and being like, this doesn’t sound like you.
DASKALAKIS: Correct. So we then asked the question, what’s going on? Can we see some kind of documentation? Because they were like, implement the change. But we’ve never seen anything in writing, so we asked if we could see the supporting data that led to the decision. And we were told no.
ABRAMS: Just flat out no?
DASKALAKIS: Flat out no.
ABRAMS: But can I ask you, did you ever actually have a conversation with Kennedy about any of this or any of his senior staffers?
DASKALAKIS: No.
ABRAMS: Or is it just that —
DASKALAKIS: No.
ABRAMS: No communication.
DASKALAKIS: No.
ABRAMS: Did you ever try?
DASKALAKIS: Yes.
ABRAMS: And what would happen?
DASKALAKIS: So we offered to do briefings when he first started. I think some people were able to brief some lower level staff, but not staff that were Secretary Kennedy’s staff. So no one from my center has ever briefed the Secretary.
ABRAMS: On anything.
DASKALAKIS: Correct, on anything.
ABRAMS: So basically, don’t have a line into RFK, and he’s not seeking out your advice or the advice of people who are theoretically supposed to advise him on things like this. How did you feel about that at the time?
DASKALAKIS: I felt that this was highly atypical, that we weren’t able to share our expertise up the chain to be able to provide information that could be meaningful and thought process. And so what I kept thinking was, we’re not doing this, but there sure is a point of view up there. I wonder who’s doing it.
My job is to make sure that we’re giving good science so people can make good decisions. And if I can’t make sure that science is untouched by non-scientific influence, I cannot say that I’m doing my job.
I believe that CDC science is going to be compromised by HHS. And if that science becomes biased, if it gets unduly influenced, then I can’t have my name on that science as something that I think should be used to make important decisions for people’s lives.
Again, I strongly recommend listening to this podcast. The other disturbing facet is the way in which Abrams just plows on; it could be an artifact of editing, but it could be another of the many ways in which media has not paused and shouted at the public how disturbing and inappropriate are RFK Jr.’s and Trump’s management of public health, in a misguided effort to remain neutral about a subject which isn’t and can’t be neutral at all.
How can a US media outlet be neutral in the face of what looks increasingly like an occupation of government agencies by hostile forces? In the case of the CDC under RFK Jr.’s HHS, it’s damaging the administration of vaccinations to the entire country while undermining the nation’s ability to respond to pandemic and bioterrorism, not to mention its ability to safely provide basic healthcare. No one will be unaffected; no one can be neutral.
~ ~ ~
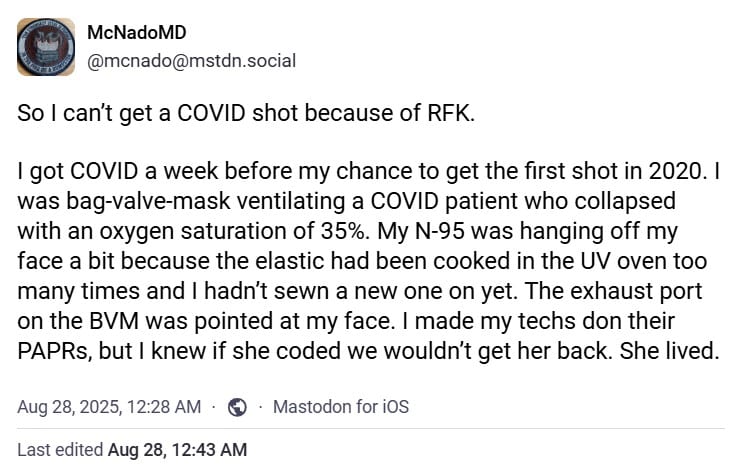
I’m not kidding when I say our healthcare is now utterly compromised. Our first responders and healthcare providers can’t be assured of necessary vaccinations. From an ER doctor on Mastodon:
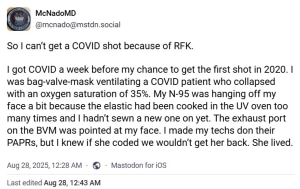
This is absolute bullshit.
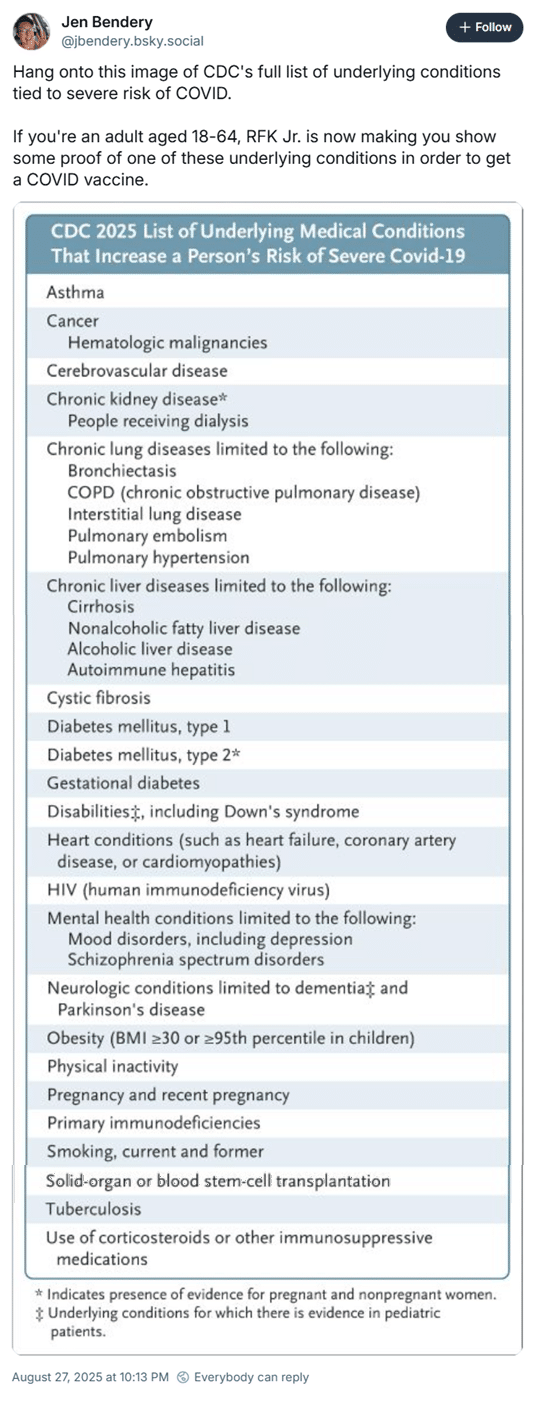
One of the biggest purveyors of anti-vaccine propaganda, one without any healthcare education and training, has decided the persons most likely to be exposed to diseases on a daily basis are no longer eligible for COVID vaccinations if they do not have a limited number of pre-existing chronic health problems. From Jen Bendery on Bluesky:
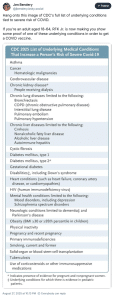
(For the record, my autoimmune disorder which has cost me lung capacity, is not on this list. I am not eligible for another COVID shot until I turn 65.)
This is a recipe for disaster. Not only are rural hospitals at risk because of cuts to Medicare under Trump’s Big Fugly Bill, all hospitals are at risk if their staff can’t be vaccinated readily in the face of a new COVID wave.
If my father were to become sick again and collapse like he did, could he be assured there would be healthcare personnel ready to receive and treat him? Or might the healthcare system be overwhelmed and triage him to the very end of the line?
The same goes for any of the rest of us, really. How can anyone in the US be assured the healthcare system will be able to respond if RFK Jr. is allowed to continue to hack away at it without supporting data, without support by seasoned, qualified professionals, without adequate oversight by Congress?
~ ~ ~
Of the many things that raced through my mind as I tried to revive my dad was the thought we had not talked about DNR status.
I’m pretty sure my dad and mom have both indicated on healthcare POAs they are DNR under certain conditions.
What happens, though, when one of them collapses at home? Should I have left him on the floor while ensuring his comfort?
Obviously I didn’t do that.
But a little over a week later I can’t help wonder if RFK Jr. has now forced DNR on swaths of Americans, and we’re already DNR where we are in our own homes whether we realize it or not.
If our healthcare system collapses because of his anti-vaccine and anti-healthcare regime, is he not assuring our healthcare system cannot resuscitate many of us?
How would this be different under a hostile foreign occupation?