These days we’re drowning in information about the pandemic, but without much context for understanding the virus causing it. With a never-before-seen virus, the best place to get that context is from looking at the history of previous diseases, and by understanding what they’ve done to our biology and society, as we try to figure out what this one does to our biology and society.

People lining up for a market in San Francisco’s Mission District
One of the first and most important questions is how Covid-19 infects people, and this disease is pretty damn infectious. Not as bad as diseases like Measles, Mumps, and Rubella, but worse than most flus. (The most infectious diseases tend to become the diseases of childhood because you’re born, and BAM! you get them, they’re so infectious.) Transmission is measured with the R₀ (“R-naught”) we keep seeing in news stories, measuring how many people one infected person will infect in a given time period. But it’s not a number that just exists without context — lowering that number is why so many of us are staying at home, trying to figure out how we’re going to pay the bills right now. But without the social distancing, Covid-19 is more infectious than anything most of us have experienced in our lives.
What makes Covid-19 infectious has a lot to do with how well the particular virus that causes it, SARS-CoV-2, survives in the world, along with how good SARS-CoV-2 is at finding the kind of cell it uses as a host and then invading it.
To contrast Covid-19 with the most recent nasty pandemic, AIDS, it is much more likely to spread and much less likely to kill those it spreads to. HIV, the virus that causes AIDS, is a delicate virus, despite causing a nasty disease. HIV dies if you blow on it.
The only fomite (the word for inanimate objects that can pass infections) that transmits HIV in the normal course of life is a needle full of HIV-infected blood, and that’s not easy to accidentally infect yourself with on your way to a restaurant. Other than direct blood transmission, it has to be transmitted person to person through intimate contact.
HIV is also good, but not great, at finding and infecting its target cells, and it happens to use the same kind of cells that Yersinia pestis, better known as the plague, and one of the worst pandemics ever, likes to invade. (This fact becomes very important in the story of contemporary civilization, hold on to your hats.)
So the limits to HIV spreading come from how hard it is for the virus to survive when it’s not in an ideal environment, and how hard it is to invade certain immune cells, its host of choice. This is why it is much easier to catch it from needle/blood transfer than anything else, and why some sex is more likely to transmit it than other sex is. For all the gay plague talk, the absolute safest sexually active group in the AIDS epidemic was lesbians. (I guess God loves lesbians the most?)
HIV is not passed via the respiratory system. The entrance to the respiratory system is the leaky liquidy parts of your face: eyes, nose, and mouth. This is an extremely important point. If HIV was transmitted that way, if it was a little hardier and could live in droplets you expel from your face, everything, and I do mean everything, would be terrible.
This isn’t because a respiratory infection couldn’t do what HIV does – there is a respiratory version of the plague that’s completely horrific. Pneumonic plague is in that category of diseases so bad that they burn themselves out by being so horrible and deadly that they run out of hosts, if not for the fact that it has other ways to spread, namely fleas. (Y. pestis is the worst.)
HIV budding out of an immune cell (NIAID)
So while HIV is terrible and has cost the world immeasurably, it’s not the plague. Also, because of the plague, HIV is considerably worse at infecting immune cells in populations that were genetically impacted by the plague. HIV uses a receptor on immune cells called CCR5. The “receptor” here is a little protein lock that opens up a cell. A bit like a tiny door with lock and doorknob. Seven hundred years before HIV came around, Y. pestis, despite being a bacterium rather than a virus, was using the same CCR5 to get inside immune cells. It killed somewhere around half of Europe and came back and kept killing for hundreds of years until the human genome declared FUCK THIS and mutated CCR5 out of service in a portion of the population, a portion that then had the chance to have more kids.
 This is why despite having similar chances to spread, HIV is less prevalent in European populations that went through that plague-induced genetic narrowing than in sub-Saharan Africa, which was probably never seriously afflicted by Y. pestis in the way Europe, western Asia, and North Africa were. This made them far more vulnerable to HIV, with the tragic results we see now.
This is why despite having similar chances to spread, HIV is less prevalent in European populations that went through that plague-induced genetic narrowing than in sub-Saharan Africa, which was probably never seriously afflicted by Y. pestis in the way Europe, western Asia, and North Africa were. This made them far more vulnerable to HIV, with the tragic results we see now.
To bring it back to our current bug: SARS-CoV-2’s infectiousness is closer to pneumonic plague than HIV in infectiousness, but also different because there’s no insect vector.
This little bugger can hang on in the environment. SARS-CoV-2 can survive for days on common surfaces like steel or plastic. It survives for four hours on copper. Copper is basically the Purell of metals. That’s not good.
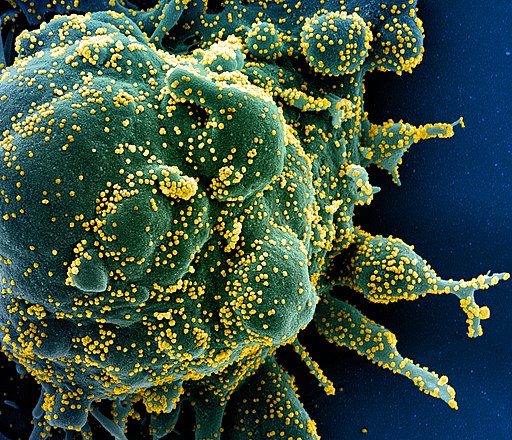
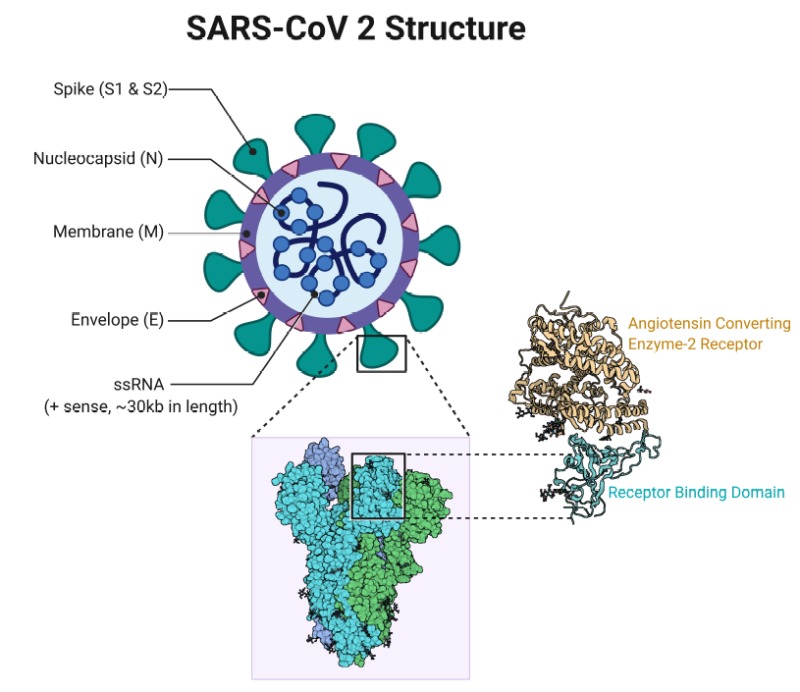
SARS-CoV-2 is very good at accessing and infecting its target cells, which are generally surface tissue (epithelial) cells with ACE2 protein receptors, analogous to the CCR5 that Y. pestis and HIV use. Anything with that ACE2 receptor will work for SAR-CoV-2, but lung cells are the tissues they most likely encounter when someone breathes in the virus. It’s harder for it to get to those same receptors in your intestines from your nose. But it’s entirely possible that for the people who do experience intestinal symptoms like diarrhea, SARS-CoV-2 got to those ACE2 receptors as well.
You can think of the ACE2 receptor as a little locked door on the surface of the cell. In order for the useful things that the cell makes to get out, or for the cell to get a useful thing it needs to get in, other cells will come by with the key that fits into the receptor and unlock it.
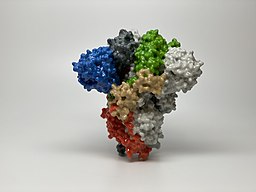
A coronavirus is a small ball of fat and protein covered in lock picks, which in this case are little “spike” proteins that fit into the ACE2 receptor and open the door for the virus’s RNA to come in.
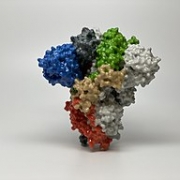
A 3D print of just the spike protein from a SARS-CoV-2 virus. This is the “lockpick” for the ACE2 receptor.
That’s it, that’s how it works. It’s amazing how much, when you get biology down to the micro level, bodies work like legos and tinker toys, but wet.
The thing about this virus, which makes it more infectious than the flu or even classic SARS or MERS, is that the spike protein on the surface of SARS-CoV-2 picks the lock of the ACE2 receptor very well. As soon as it hits it, it locks in. That means fewer viruses are needed to infect a person.
That, along with how well it survives and travels in droplets, is what stopped the world.
The good news is for most people Covid-19 doesn’t do much. In many cases, it does even less than the flu or a normal cold. It’s good news for people who get Covid-19, but not great news for a planet trying to find and isolate asymptomatic cases. You win some, you lose some.
There are two kinds of immune systems at play in responding to anything that threatens the body: the innate immune system, and the adaptive immune system.
The innate is your first level of defense, looking for and eliminating baddies like SARS-CoV-2. But the innate system isn’t where you get immunity. Immunity comes from a process where the innate system reacts to a novel bug it has never seen, and learns about it. Then a certain kind of innate immune cell, called a dendritic cell, presents the shape of a coronavirus, or whatever other nasty pathogen the body is fighting, to the T and B cells of the adaptive immune system, which then go all Terminator and hunt down and kill whatever is shaped like the thing they got from the innate system.
That process is what we call acquiring immunity, and it’s why no one can, by definition, be immune to a novel virus, including this one. Immune is not the same as showing no symptoms, even though many people, including journalists, keep using those terms interchangeably. That is a dangerous mistake, so let me repeat this: the only people on our beloved blue-green world who are immune to Covid-19 are those who have had it and recovered from it, and we’re not even sure how immune they are. So why do some people seem immune?
Covid-19 seems to have some way of calming down some innate immune responses (mechanisms which seem work strangely in children, that’s still unclear). It doesn’t usually win against the learned immune response in most people who get infected, who clear out the virus and become immune. Of course, this isn’t how it goes for everyone… but thankfully for most of us, it’s mild to asymptomatic.
The problem is with the virus calming the innate immune response is that the innate immune system is what gives you symptoms. Viruses don’t give you fevers and headaches, coughs, aches, and the desire to stay in bed, your immune response does that.
Without those symptoms infected people spread this very hardy virus all over until the immune system catches up with making them feel sick. We don’t know how long asymptomatic carriers shed virus this way. It could be a day, it could be two weeks.
In the end, it’s likely most of us are either going to get Covid-19 or get a vaccine. With this much global spread, the disease is headed to be the next coronoavirus to be endemic in humanity (the common cold is caused by other coronaviruses between 15-20% of the time).
Endemic means this is a disease the floats around the population, with pretty much one infected person infecting one more person (R=1). Many endemic diseases in history are nasty, like Smallpox, which in its prime regularly killed a third of children in Europe.
Endemic diseases can also flare into epidemics, when they encounter a large group of people without immunity, and then calm down again once they’ve done their damage. Diseases going from epidemic to endemic don’t just change our lifestyles and our societies, they change us at the genetic level, and we change them back.
We see that with the HIV and plague connection, and with European explorers accidentally (mostly) wiping out the vast majority of the new world, for whom the Smallpox virus was, like Covid-19, novel, and consequently far more deadly.
I hope we get the vaccine, and the news is good there, so far. SARS-CoV-2 doesn’t seem to be a fast mutator, unlike HIV, which has dodged all of our attempts to vaccinate for it.
Covid-19 might be treatable with some kind of antiviral medications, which would be nice, but that needs to go through trials first before any more unscrupulous doctors and incompetent politicians make up things about malaria meds, and people start eating fish tank cleaner en masse.
But in general, this is a bit like plague-level nightmare transmission, but with novel influenza lethality. Not great, but it could be much worse. At its most terrible, Y. pestis could kill up to 80% of its victims. (Y. pestis is the worst.)
How long we stay immune is another question, and we are far from answering it.
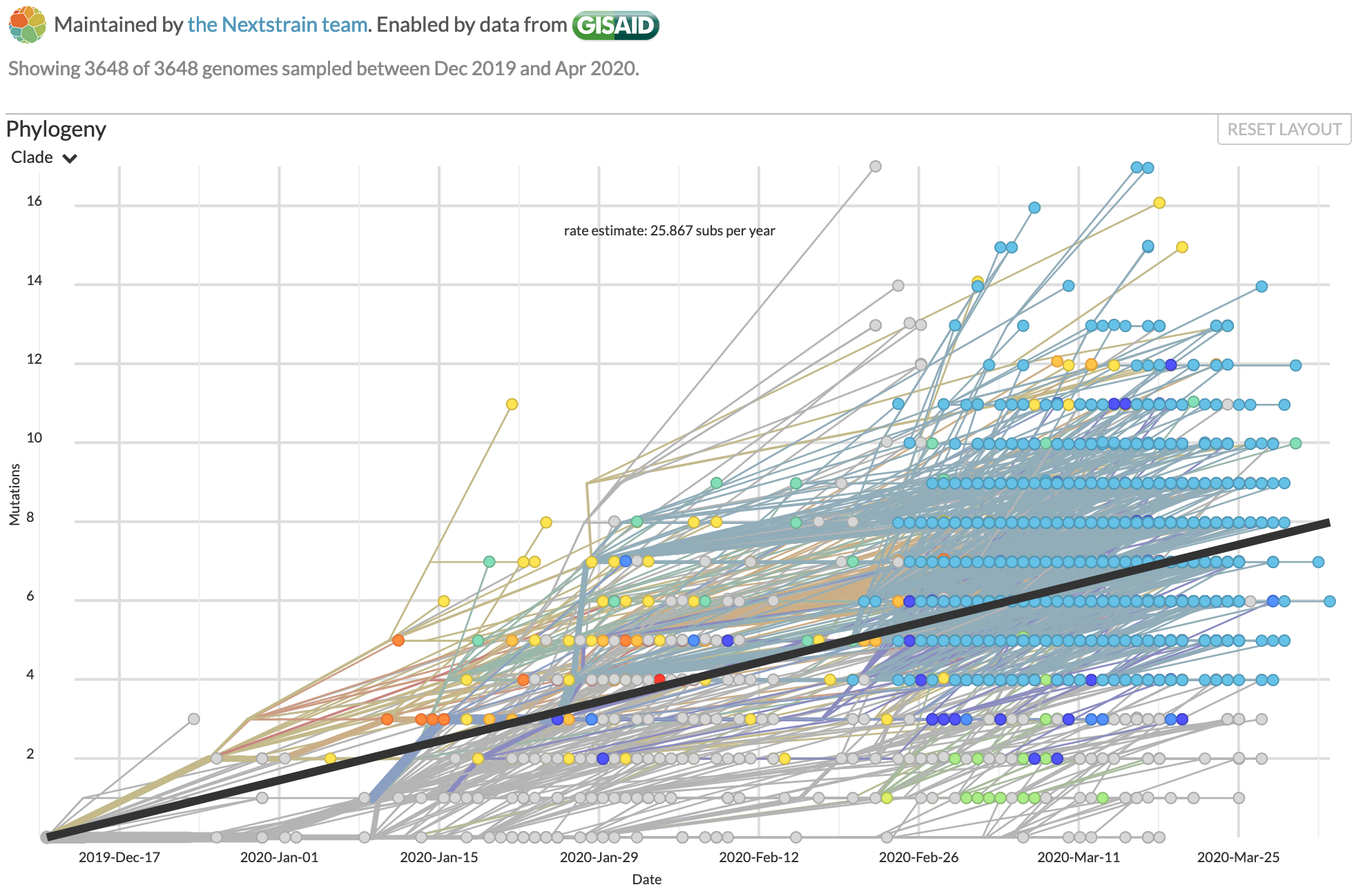
There’s two factors at play – one is that some immunity (like Smallpox) is for life, but for some other diseases, the adaptive immune system forgets about them after enough time passes. The second factor is how much the virus changes as it mutates going through hosts. The more people it infects, the more chances there are for the virus’s genes to drift as it reproduces. That makes more chances for it to become different enough that the body has to learn about it again, which unfortunately gets done by getting re-infected. It’s early days, but so far SARS-CoV-2 doesn’t seem to be prone to drifting.
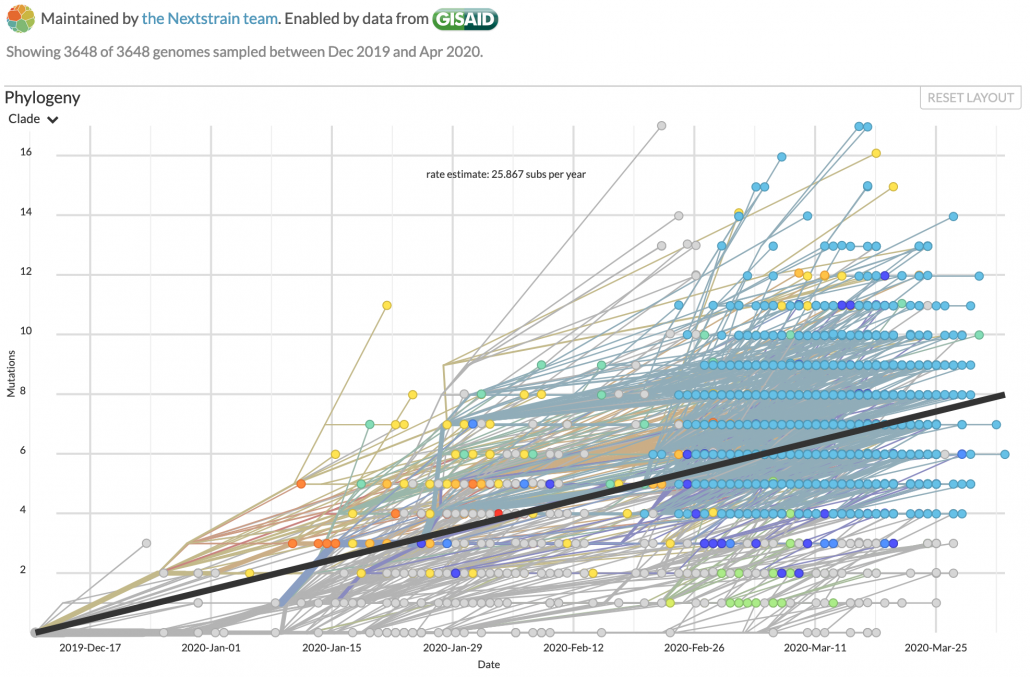
Genomic changes in SARS-CoV-2 as it infects the world, tracked by Nextstrain.
SARS-CoV-2’s apparent genetic stability is some of the best news we’ve had for beating this disease in the long term, but it’s still early days. When bugs become endemic, they tend to lose some of their virulence as well. Killing your hosts isn’t very adaptive for a parasite, and dying isn’t very adaptive for us. But that is generations away.
For now, keep washing your hands and staying home for everything but essential work, store runs, exercise, and medical care. This is going to be very hard for everyone, but humanity will get through it together.
My work for Emptywheel is supported by my wonderful patrons on Patreon. You can find out more, and support my work, at Patreon.