Understanding Covid-19 for Viral Newbies
These days we’re drowning in information about the pandemic, but without much context for understanding the virus causing it. With a never-before-seen virus, the best place to get that context is from looking at the history of previous diseases, and by understanding what they’ve done to our biology and society, as we try to figure out what this one does to our biology and society.

People lining up for a market in San Francisco’s Mission District
One of the first and most important questions is how Covid-19 infects people, and this disease is pretty damn infectious. Not as bad as diseases like Measles, Mumps, and Rubella, but worse than most flus. (The most infectious diseases tend to become the diseases of childhood because you’re born, and BAM! you get them, they’re so infectious.) Transmission is measured with the R₀ (“R-naught”) we keep seeing in news stories, measuring how many people one infected person will infect in a given time period. But it’s not a number that just exists without context — lowering that number is why so many of us are staying at home, trying to figure out how we’re going to pay the bills right now. But without the social distancing, Covid-19 is more infectious than anything most of us have experienced in our lives.
What makes Covid-19 infectious has a lot to do with how well the particular virus that causes it, SARS-CoV-2, survives in the world, along with how good SARS-CoV-2 is at finding the kind of cell it uses as a host and then invading it.
To contrast Covid-19 with the most recent nasty pandemic, AIDS, it is much more likely to spread and much less likely to kill those it spreads to. HIV, the virus that causes AIDS, is a delicate virus, despite causing a nasty disease. HIV dies if you blow on it.
The only fomite (the word for inanimate objects that can pass infections) that transmits HIV in the normal course of life is a needle full of HIV-infected blood, and that’s not easy to accidentally infect yourself with on your way to a restaurant. Other than direct blood transmission, it has to be transmitted person to person through intimate contact.
HIV is also good, but not great, at finding and infecting its target cells, and it happens to use the same kind of cells that Yersinia pestis, better known as the plague, and one of the worst pandemics ever, likes to invade. (This fact becomes very important in the story of contemporary civilization, hold on to your hats.)
So the limits to HIV spreading come from how hard it is for the virus to survive when it’s not in an ideal environment, and how hard it is to invade certain immune cells, its host of choice. This is why it is much easier to catch it from needle/blood transfer than anything else, and why some sex is more likely to transmit it than other sex is. For all the gay plague talk, the absolute safest sexually active group in the AIDS epidemic was lesbians. (I guess God loves lesbians the most?)
HIV is not passed via the respiratory system. The entrance to the respiratory system is the leaky liquidy parts of your face: eyes, nose, and mouth. This is an extremely important point. If HIV was transmitted that way, if it was a little hardier and could live in droplets you expel from your face, everything, and I do mean everything, would be terrible.
This isn’t because a respiratory infection couldn’t do what HIV does – there is a respiratory version of the plague that’s completely horrific. Pneumonic plague is in that category of diseases so bad that they burn themselves out by being so horrible and deadly that they run out of hosts, if not for the fact that it has other ways to spread, namely fleas. (Y. pestis is the worst.)
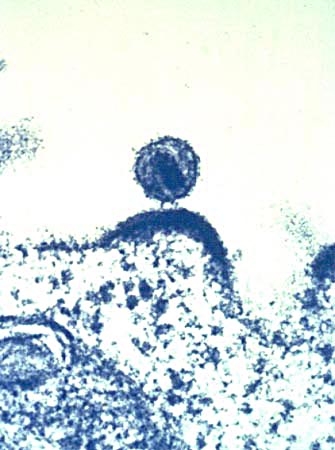
HIV budding out of an immune cell (NIAID)
So while HIV is terrible and has cost the world immeasurably, it’s not the plague. Also, because of the plague, HIV is considerably worse at infecting immune cells in populations that were genetically impacted by the plague. HIV uses a receptor on immune cells called CCR5. The “receptor” here is a little protein lock that opens up a cell. A bit like a tiny door with lock and doorknob. Seven hundred years before HIV came around, Y. pestis, despite being a bacterium rather than a virus, was using the same CCR5 to get inside immune cells. It killed somewhere around half of Europe and came back and kept killing for hundreds of years until the human genome declared FUCK THIS and mutated CCR5 out of service in a portion of the population, a portion that then had the chance to have more kids.
 This is why despite having similar chances to spread, HIV is less prevalent in European populations that went through that plague-induced genetic narrowing than in sub-Saharan Africa, which was probably never seriously afflicted by Y. pestis in the way Europe, western Asia, and North Africa were. This made them far more vulnerable to HIV, with the tragic results we see now.
This is why despite having similar chances to spread, HIV is less prevalent in European populations that went through that plague-induced genetic narrowing than in sub-Saharan Africa, which was probably never seriously afflicted by Y. pestis in the way Europe, western Asia, and North Africa were. This made them far more vulnerable to HIV, with the tragic results we see now.
To bring it back to our current bug: SARS-CoV-2’s infectiousness is closer to pneumonic plague than HIV in infectiousness, but also different because there’s no insect vector.
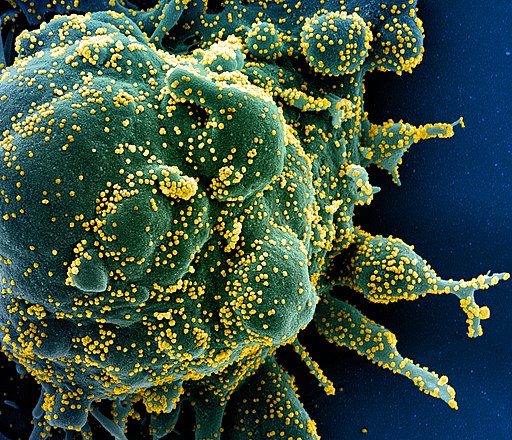
This little bugger can hang on in the environment. SARS-CoV-2 can survive for days on common surfaces like steel or plastic. It survives for four hours on copper. Copper is basically the Purell of metals. That’s not good.
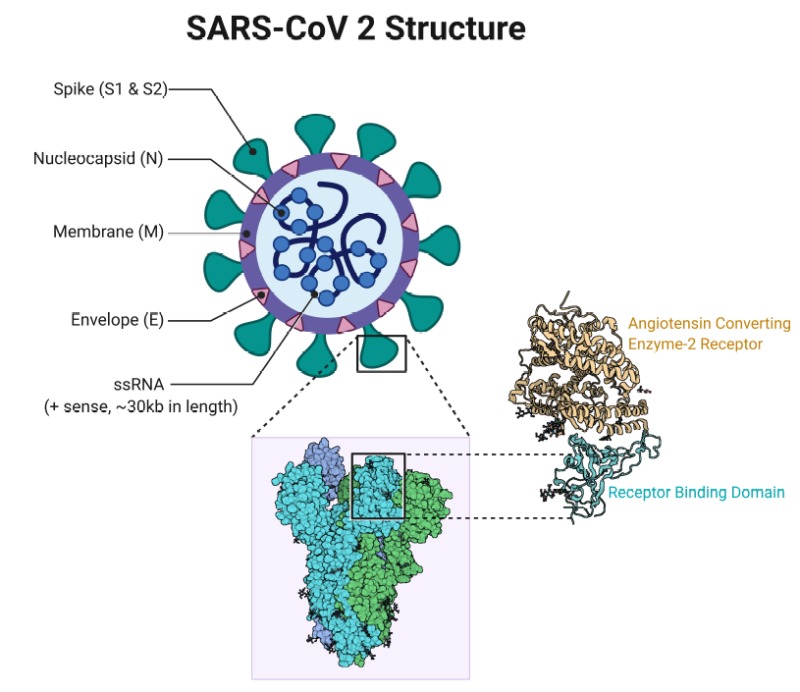
SARS-CoV-2 is very good at accessing and infecting its target cells, which are generally surface tissue (epithelial) cells with ACE2 protein receptors, analogous to the CCR5 that Y. pestis and HIV use. Anything with that ACE2 receptor will work for SAR-CoV-2, but lung cells are the tissues they most likely encounter when someone breathes in the virus. It’s harder for it to get to those same receptors in your intestines from your nose. But it’s entirely possible that for the people who do experience intestinal symptoms like diarrhea, SARS-CoV-2 got to those ACE2 receptors as well.
You can think of the ACE2 receptor as a little locked door on the surface of the cell. In order for the useful things that the cell makes to get out, or for the cell to get a useful thing it needs to get in, other cells will come by with the key that fits into the receptor and unlock it.
A coronavirus is a small ball of fat and protein covered in lock picks, which in this case are little “spike” proteins that fit into the ACE2 receptor and open the door for the virus’s RNA to come in.
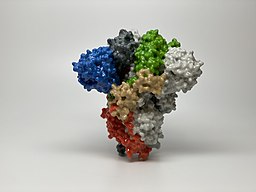
A 3D print of just the spike protein from a SARS-CoV-2 virus. This is the “lockpick” for the ACE2 receptor.
That’s it, that’s how it works. It’s amazing how much, when you get biology down to the micro level, bodies work like legos and tinker toys, but wet.
The thing about this virus, which makes it more infectious than the flu or even classic SARS or MERS, is that the spike protein on the surface of SARS-CoV-2 picks the lock of the ACE2 receptor very well. As soon as it hits it, it locks in. That means fewer viruses are needed to infect a person.
See more here.
That, along with how well it survives and travels in droplets, is what stopped the world.
The good news is for most people Covid-19 doesn’t do much. In many cases, it does even less than the flu or a normal cold. It’s good news for people who get Covid-19, but not great news for a planet trying to find and isolate asymptomatic cases. You win some, you lose some.
There are two kinds of immune systems at play in responding to anything that threatens the body: the innate immune system, and the adaptive immune system.
The innate is your first level of defense, looking for and eliminating baddies like SARS-CoV-2. But the innate system isn’t where you get immunity. Immunity comes from a process where the innate system reacts to a novel bug it has never seen, and learns about it. Then a certain kind of innate immune cell, called a dendritic cell, presents the shape of a coronavirus, or whatever other nasty pathogen the body is fighting, to the T and B cells of the adaptive immune system, which then go all Terminator and hunt down and kill whatever is shaped like the thing they got from the innate system.
That process is what we call acquiring immunity, and it’s why no one can, by definition, be immune to a novel virus, including this one. Immune is not the same as showing no symptoms, even though many people, including journalists, keep using those terms interchangeably. That is a dangerous mistake, so let me repeat this: the only people on our beloved blue-green world who are immune to Covid-19 are those who have had it and recovered from it, and we’re not even sure how immune they are. So why do some people seem immune?
Covid-19 seems to have some way of calming down some innate immune responses (mechanisms which seem work strangely in children, that’s still unclear). It doesn’t usually win against the learned immune response in most people who get infected, who clear out the virus and become immune. Of course, this isn’t how it goes for everyone… but thankfully for most of us, it’s mild to asymptomatic.
The problem is with the virus calming the innate immune response is that the innate immune system is what gives you symptoms. Viruses don’t give you fevers and headaches, coughs, aches, and the desire to stay in bed, your immune response does that.
Without those symptoms infected people spread this very hardy virus all over until the immune system catches up with making them feel sick. We don’t know how long asymptomatic carriers shed virus this way. It could be a day, it could be two weeks.
In the end, it’s likely most of us are either going to get Covid-19 or get a vaccine. With this much global spread, the disease is headed to be the next coronoavirus to be endemic in humanity (the common cold is caused by other coronaviruses between 15-20% of the time).
Endemic means this is a disease the floats around the population, with pretty much one infected person infecting one more person (R=1). Many endemic diseases in history are nasty, like Smallpox, which in its prime regularly killed a third of children in Europe.
Endemic diseases can also flare into epidemics, when they encounter a large group of people without immunity, and then calm down again once they’ve done their damage. Diseases going from epidemic to endemic don’t just change our lifestyles and our societies, they change us at the genetic level, and we change them back.
We see that with the HIV and plague connection, and with European explorers accidentally (mostly) wiping out the vast majority of the new world, for whom the Smallpox virus was, like Covid-19, novel, and consequently far more deadly.
I hope we get the vaccine, and the news is good there, so far. SARS-CoV-2 doesn’t seem to be a fast mutator, unlike HIV, which has dodged all of our attempts to vaccinate for it.
Covid-19 might be treatable with some kind of antiviral medications, which would be nice, but that needs to go through trials first before any more unscrupulous doctors and incompetent politicians make up things about malaria meds, and people start eating fish tank cleaner en masse.
But in general, this is a bit like plague-level nightmare transmission, but with novel influenza lethality. Not great, but it could be much worse. At its most terrible, Y. pestis could kill up to 80% of its victims. (Y. pestis is the worst.)
How long we stay immune is another question, and we are far from answering it.
There’s two factors at play – one is that some immunity (like Smallpox) is for life, but for some other diseases, the adaptive immune system forgets about them after enough time passes. The second factor is how much the virus changes as it mutates going through hosts. The more people it infects, the more chances there are for the virus’s genes to drift as it reproduces. That makes more chances for it to become different enough that the body has to learn about it again, which unfortunately gets done by getting re-infected. It’s early days, but so far SARS-CoV-2 doesn’t seem to be prone to drifting.
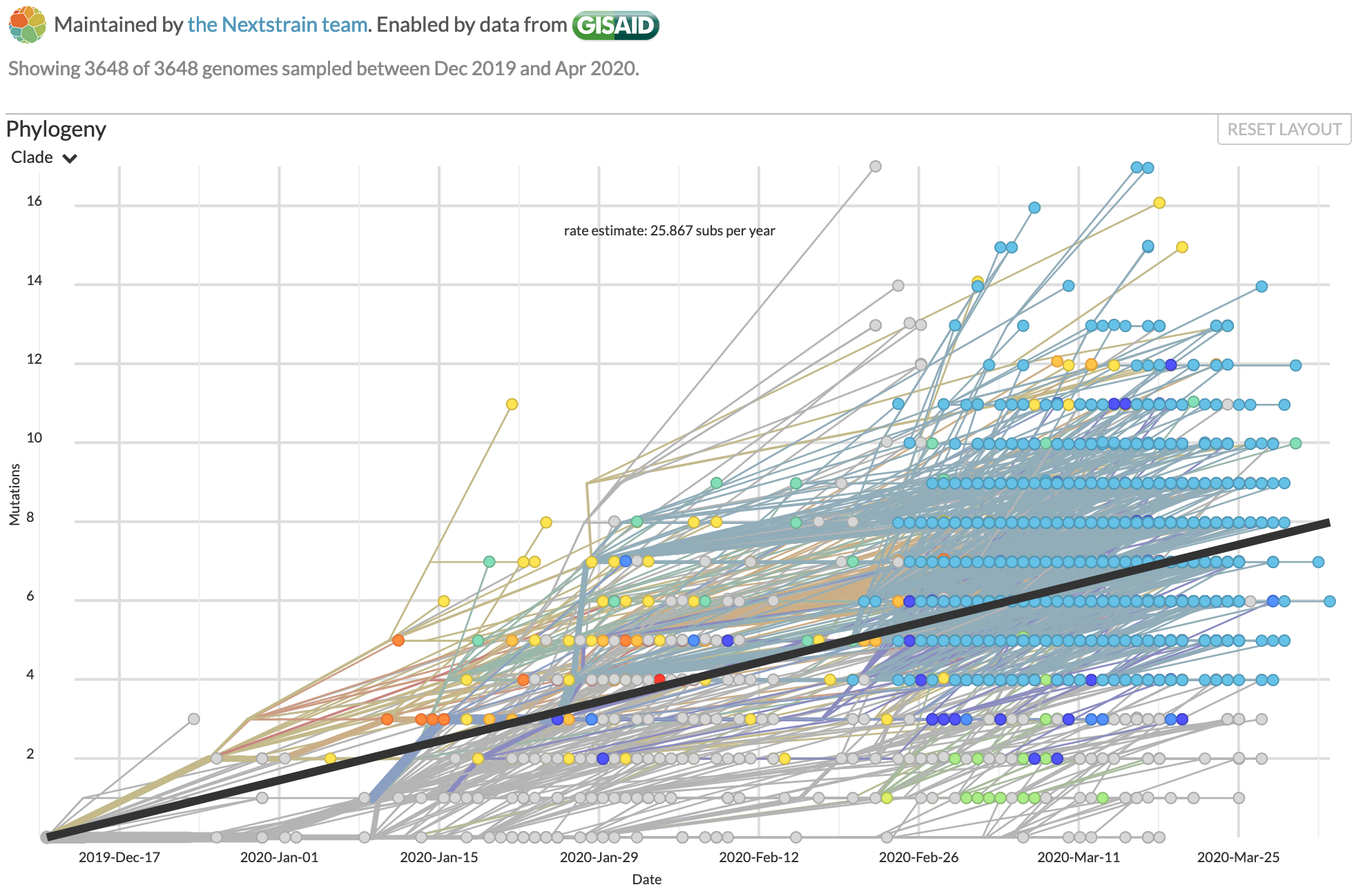
Genomic changes in SARS-CoV-2 as it infects the world, tracked by Nextstrain.
SARS-CoV-2’s apparent genetic stability is some of the best news we’ve had for beating this disease in the long term, but it’s still early days. When bugs become endemic, they tend to lose some of their virulence as well. Killing your hosts isn’t very adaptive for a parasite, and dying isn’t very adaptive for us. But that is generations away.
For now, keep washing your hands and staying home for everything but essential work, store runs, exercise, and medical care. This is going to be very hard for everyone, but humanity will get through it together.
My work for Emptywheel is supported by my wonderful patrons on Patreon. You can find out more, and support my work, at Patreon.



The UK’s prime minister, Boris Johnson, was moved to ICU today. The survival rate in the UK for those moved to ICU is about fifty percent. The rapidity of the downturn seems typical of those who experience it, as is the timing, 10-11 days after onset of symptoms.
In explaining his rapid downturn, the media has discussed Johnson’s weight as a potential contributing factor in his susceptibility to a more extreme case. It has not discussed Johnson’s decades’ long reputation – whether true or not – for living to excess, particularly his reputed consumption of alcohol and recreational drugs.
honestly from looking at how this bug behaves, my guess would be weight for sure, but alcohol really would require deep alcoholism, and recreational drugs probably make no difference at all.
Would damage to lungs from, say, lighting things on fire and inhaling them make a person more susceptible? Or would the existing damage make recovery more difficult?
Asking as a fan of recreational drugs.
I don’t know, but the shops in CA are reporting more people getting edibles these days.
A report this morning on NPR said that the serious cases seen in some younger people may be because vaping and smoking weed/cigarettes has set some of them up with an invisible ‘pre-existing condition’ in their lungs. This is an area that is being investigated now.
Mediterranean countries like Italy and Spain have a higher smoking rate than northern Europe, as well as a higher percentage of elderly people.
My memory of Italy was that men smoked more than women also.
There’s a lot of smoking in east Asia, also – mostly men, I think.
In Korea the gender disparity for smokers is extreme (like 40% to 5%), but I haven’t seen any data about the gender balance of COVID victims there.
http://ncov.mohw.go.kr/bdBoardList_Real.do?brdId=1&brdGubun=11&ncvContSeq=&contSeq=&board_id=&gubun=
says: 2.44% CFR for males, 1.47% for females.
That doesn’t say too much though without also having the age distributions, which I don’t have.
smoking is def going to make all of this worse, and nicotine is a nightmare, but most (other) recreational drugs aren’t indulged in as frequently as smoking is, and are probably not as bad as smoking. whether this accounts for the gender disparity in outcomes… who knows! isn’t novel fun?
I am fan of the kinds of recreational drugs that must be lit. I am also an occasional tobacco user. When I first became aware of this virus, I started to note every time I touched my hands to my face, so I could recognize and avoid it, and found that it was well-nigh impossible to smoke a joint or cigarette without touching my face multiple times or fiddling with the end that goes in my mouth. I’d be really surprised if heavy smoking didn’t make the effects of any respiratory virus, including this one, more severe. But I suspect that the biggest risk of smoking is contracting the virus in the first place, because of the hand/mouth contact involved.
If I had any of the recreational product (sadly, the nearest dispensary isn’t within walking distance), I’d use a pipe. For that occasional (I have at most one or two a day) tobacco cigarette, I wash my hands thoroughly before extracting the tube from the (disinfected) pack and use an alligator clip, affixed well away from the filter, to bring it to my mouth. Maybe this will help me give up my rather minor habit, because I really did enjoy the fiddling, even more than the actual tobacco buzz.
I’d really suggest giving up all smoking and maybe do edibles for fun instead.
The risk is less that you’re touching your face so much. I don’t want to get technical about it but it’s the damage you’ve done to your lungs smoking and what the virus will do to your lungs whether you infect yourself by touching your face or inhale an infected person’s exhalations.
had a scan done on my lungs a couple of years ago GP wasn’t amuzed. the damage has been done. although I have’t smoked since 96 there is damage and its not going to get better, by quitting its not going to get worse though. did save a lot of money thiough by quitting. I quit when it was $3.60 a pack. now its about $15 a pack.
The damage this virus does to lungs is hideous. It’s the reason I dare take no chances because of lung damage from an autoimmune disorder.
Yes, of course. Inhaling smoke is never good for the lungs. Never.
Having been a smoker, it’s my devout hope that enough time has passed that, should this come my way, my lungs will have recovered enough to not be severely effected.
It’s never too late to quit! If I can, so can anyone.
And there are other ways to ingest whatever you’re ingesting.
(Except tobacco. There’s no good way to ingest tobacco or even nicotine, which is toxic in many ways.)
I could see Mr Johnson on a precedex drip.
The reaper comes for what was sowed.
These brutal cuts to the NHS will haunt the Conservatives
https://www.theguardian.com/commentisfree/2019/oct/25/boris-johnson-conservatives-nhs-funding
Excessive weight as in metabolic syndrome, which implicates the immune system? That would not be good news for the US population and others that have adopted the American industrial diet (the UK included). Unfortunately, the US has seen consistent high growth in the incidence of metabolic syndrome, which includes obesity.
Yes, it’s really not good news. We’ll see. :(
Trying to get the morbidly obese off the ventilator is one of the banes of my specialty. Not easily done. BMI of greater than 35 has profound effects on your lungs and ability to breathe.
Thanks for posting this.
Thanks to Quinn Norton for taking the time to write this.
Y. pestis isn’t immune to antibiotics, though, being a bacterium, not a virus. (One point in our favor.)
Thanks for the article. DR in totality for now. The ending has:
“When bugs become endemic, they tend to lose some of their virulence as well. Killing your hosts isn’t very adaptive for a parasite, and dying isn’t very adaptive for us. But that is generations away.”
The bugs generational life-span is measured in hours. Humans is generally measured in 20-30 years. Guess the bugs will outsmart us on the genetic adaptation scale bigly.
Thanks for the interesting read, Quinn. I’ve been thinking about some of these things lately. It brings to mind a lengthy article from a few years ago that caught my attention. Here are some excerpts and the url:
“Medicine’s Movable Feast: What Jumping Genes Can Teach Us about Treating Disease”
“Ancient viruses “fossilized” in the genome may contribute to maladies from autoimmune diseases to schizophrenia”
Roxanne Khamsi, July 26, 2017
…..
“Although experts remain skeptical that a virus will integrate into the human genome again anytime soon, other transposable elements, such as LINE-1s, continue to move around in our DNA. Meanwhile, the field that Barbara McClintock seeded more than half a century ago is growing quickly.”
“John Abrams, who is studying retroelements, says that we’re only just beginning to understand how dynamic the genome is. He notes that only recently have people begun to appreciate how the ‘microbiome’ of bacteria living in our guts can influence our health. “We’re really an ecosystem,” Abrams says of the gut, “and the genome is the same way.” There is the host DNA—belonging to us—and the retro-elements it contains, he explains, and “there’s this sort of productive tension that exists between the two.””
https://www.scientificamerican.com/article/medicines-movable-feast-what-jumping-genes-can-teach-us-about-treating-disease/
Very edifying Quinn, thank you.
NPR is reporting a “Promising Drug On The Horizon For COVID-19”
They say the drug is known as EIDD-2801. It works by interfering with the coronavirus’ ability to make copies of itself once it infects a cell. In that regard it’s similar to remdesivir, a drug currently being tested in COVID-19 patients.
EIDD-2801 has one major advantage over remdesivir: It can be taken as a pill, whereas remdesivir must be given intravenously.
https://www.npr.org/sections/coronavirus-live-updates/2020/04/06/828322576/promising-drug-on-the-horizon-for-covid-19
This is very solid and interesting work, but they’ve only tested it in mice so far, so don’t get too excited about it. The author who said that you could potentially leap-frog testing on non-human primates and use this as a compassionate use therapy for COVID-19 is correct, but this is the kind of drug that I’d be cautious about if I were the FDA, especially since remdesivir is currently in trials. The drug trials with fialuridine, a drug that has a similar mechanism of action, did not end well:
https://en.wikipedia.org/wiki/Fialuridine
For more on the importance of full testing, see also “Thalidomide, history of”:
The numbers are almost certainly artificially low. Governments went out of their way to hide them and to protect themselves from liability, especially those that directly funded their health care systems. The UK was and remains notorious in this regard.
John Pilger edited an anthology about daring reporters and the stories their governments did not want covered: Tell Me No Lies: Investigative Journalism and Its Triumphs (2004). It has a section on the thalidomide scandal. He also produced a documentary about it.
The Guardian in 2016 wrote that the drug probably led to 10,000 infant deaths in the UK alone. It estimated worldwide deaths at 80,000, and severe abnormalities at 20,000. Below is a barebones timeline of the scandal in the UK.
https://www.theguardian.com/society/2016/mar/06/thalidomide-caused-up-to-10000-miscarriages-infant-deaths-uk
https://www.theguardian.com/society/2012/sep/01/thalidomide-scandal-timeline
Thalidomide was also a rude awakening about synthetics versus natural drugs, since natural thalidomide (there is such a thing) has another enantiomer (think of right and left hands, courtesy of some double bonds in the molecule preventing rotation) which is similar but doesn’t act exactly the same in the body. However, the stereochemistry wasn’t examined for the synthesized version and that is why many of the deformations occurred.
Its tragedy why the FDA (used to) enforce safety and effectiveness for drugs in the USA.
The deadly after-effects of thalidomide on female children born to mother’s who took the drug continue to this day:
https:// http://www.independent.co.uk/life-style/health-and-families/health-news/thousands-of-women-could-be-at-risk-from-silent-thalidomide-6292889.html
This is exactly what I thought of when considering trump’s pharma-flogging.
My mother suffered from severe nausea and vomiting while she was pregnant with me, was offered the stuff, and thank god refused it.
Thalidomide also saw some off label use in the therapy of leprosy and certain cancers. Iirc its badly supervised use for leprosy in South America caused a new wave of afflicted children.
I have a lot of hope for those kind of interfering drugs, but it’s still very early days, and that whole style of attack has one major downside: it also interferes with the body’s replication of RNA, which can be Very Bad News in the side effect department. That really limits its usefulness as an early intervention or a prophylactic, since at the time that it’s most important, you often can’t know which will be deadlier, the disease or the intervention.
Good article; thank you so much. A couple follow up questions.
We know that for some diseases, like measles or the flu, some people simply do not “get” (suffer from) that disease, period, even when seriously exposed (Contagion’s Matt Damon is today’s exemplar). What does that mean? Does that mean that their bodies are such that the virus does not get into their cells? Or does it mean that it does get into the cells, but then nothing bad happens as a result?
And how does a vaccine work? Does it stop the virus from entering the cells? Or does it stop the bad things from happening afterward?
The people who do not “get” do absolutely get it, it gets into their cells and everything, they just don’t have symptoms. Contagion actually does this well, but subtly — the perfectly fine Matt Damon is held in isolation and no one can see him without full PPE, because he’s shedding virus and able to infect people the whole time. (except for eye protection they absolutely didn’t portray eye protection right, arg!)
A lot happens in the bodies of everyone when they get this virus, but not everyone feels anything as a result. The innate system finds it and presents data about it to the adaptive system, and then the adaptive system finds the viruses and kills them. It will do that every time the virus gets into the body again, as well.
A vaccine basically causes that second part of the immune response to happen: it shows the part of the virus to the body, and eventually to the T and B cells, in the same way getting the virus would. Sometimes that causes the innate immune response to kick off a bit, that’s why you sometimes get soreness, headaches, and a fever after a flu shot.
Thank you for this.
Even the asymptomatics appear to have the “ground glass” appearance in their lungs with CT, so they may not feel any symptoms with normal activity but the next time they try to run 10km, it may feel like they have lost a liter of blood (or maybe not, too soon to say…but the CT scans do indicate some pathology).
The ground glass opacities on CT are not likely to be asymptomatic. As you point out the ground glass would lead to shortness of breath during activity. CT is can miss interstitial lung disease (a known cause of ground glass] that a lung biopsy may pick up.
That ground glass opacity showing on the CTs definitely indicates limited breathing capacity. Due to dapsone hypersensitivity syndrome I suffered with that lasted for several months, before a bronchoscopy with biopsy which revealed the lung tissue had become friable – the tissue broke off on excision. That was almost 20 years ago and my lungs have not been quite the same since, as I already had asthma by then.
Maybe they’re just pre-symptomatic. From the study of the passengers on the Diamond Princess (https://pubs.rsna.org/doi/10.1148/ryct.2020200110), the authors say, “Of 104 cases, 76 (73%) were asymptomatic, 41 (54%) of which had lung opacities on CT. Other 28 (27%) cases were symptomatic, 22 (79%) of which had abnormal CT findings. Symptomatic cases showed lung opacities and airway abnormalities on CT more frequently than asymptomatic cases [lung opacity; 22 (79%) vs 41 (54%), airway abnormalities; 14 (50%) vs 15 (20%)]. Asymptomatic cases showed more GGO over consolidation (83%), while symptomatic cases more frequently showed consolidation over GGO (41%).” So better CTs in the asymptomatic group but still showing ground glass.
I can’t find the reference now, but I’m sure there was an early report from China describing children who were asymptomatic but RNA positive and showed ground glass on CT. I could be mis-remembering, though.
So, ggo’s can be totally asymptomatic. A great example of this is adenocarcinoma in situ of the lung which appears as ggo’s (usually 1-3) in the lungs and patients have no idea they have lung cancer. The only way this is picked up is incidentally on a chest CT or through a dedicated screening program.
A ggo means that there is some sort of cellular infiltrate in the terminal bronchioles and alveoli (air sacs). Could be cancer, could be immune cells, could be some other type of cell. It’s very patchy and involves a very small portion of the lung, so it’s absolutely possible that there is no change to overall blood oxygen levels, or any sort of feeling of shortness of breath.
Consolidation, on the other hand, will likely be only in those who are symptomatic. Consolidation represents the filling of the alveoli and the small airways with fluid. Usually there’s interstitial (meaning the tissue spaces between the air sacs) fluid as well, which is being forced out of the small blood vessels due to increased pressure in the vessels from the heart getting backed up, or because the vessels are made “leaky” from inflammation and tissue damage from the infection.
John Marshall reports that Illinois’s governor, J. B. Pritzker, confirms that USG “Air Bridge” flights are bringing in PPE from China to the US. Trump’s government is handing it to private sector companies, leaving states to bid against each other to buy it from them, presumably at price gouging levels. https://twitter.com/joshtpm/status/1247335425074696199
Meanwhile, the two largest hospital systems operating in Detroit – Beaumont Health and Henry Ford Health – report over 2200 of their employees have tested positive for Covid-19. https://eu.detroitnews.com/story/news/local/michigan/2020/04/06/over-600-henry-ford-health-workers-test-positive-covid-19/2955929001/
Trump is personally carving out a new level of hell for himself and his friends, especially Moscow Mitch and Finger-on-the-Scale John Roberts and his conservative brethren. Beyond that, words fail me.
Apologies: Josh Marshall.
I’m thinking pitchforks and torches. Maybe for the 4th. For everyone who’s backing Trmp in DC.
More details from Josh Marshall, from 22.06 this evening. https://talkingpointsmemo.com/edblog/more-details-on-airlifts-and-supply-seizures
It appears that Trump – or Jared Kushner’s private sector task force – has concluded that the USG has no capacity to distribute its own resources without private sector assistance, and a piece of the action. Something tells me that the raw data alone those companies will acquire from this exercise would be worth the price of admission.
They’re certainly going to make money doing it that way. But they’re stealing from states (and even other countries), which is a crime.
Grossly, it’s the standard neoliberal model for government. Jared is simply following a well-trodden path.
Neoliberals define government as their exclusive food trough. It exists solely to serve the private sector. Its most efficient attribute is that it has the exclusive power to make laws – and to refuse to make those that might restrict profit-taking – and the exclusive power to enforce them, ultimately through physical violence.
The DoD, for example, can’t let service members eat, pee, wash, arm themselves, or go to war until some private sector company has prepared the way and comes along with them.
That trend started when Dick Cheney was SecDef, but picked up rapidly when Donald Rumsfeld was SecDef and he was Vice President. It’s pretty much metastasized across government. Trump’s “management” of his Covid-19 response – and apparently his personal profit-taking from it – are just the latest examples.
The USA can’t afford to wait for; trump to go to hell.;;.the country can not wait that long; I’d be happier if he caught a good case of COVID 19. now I understand its like breathing glass. a few weeks of that and then we can talk again.
I’ve been praying for that from the start! It would be poetic justice indeed!
Public health performance art in North Philadelphia:
“Philly really different 😂… ”
https://twitter.com/Aaliyahhhs/status/1247207920909144072
Also a local company (the one Trump couldn’t/didn’t name –?–…) started first human injections in a vaccine trial (phase aims to reach N=40, split between Philadelphia and Kansas City <– the one in MO, not KS) (that last aside was for POTUS & friends).
https://www.inquirer.com/health/coronavirus/coronavirus-covid19-vaccine-dose-volunteers-philadelphia-20200406.html
From The Daily Beast “Trump Has ‘Financial Interest’ in Hydroxychloroquine Manufacturer: NYT”:
President Donald Trump has a “small financial interest” in the maker of an anti-malarial drug that he has been touting as a “game changer” in treating coronavirus, according to The New York Times. Over the past two weeks, Trump and his Fox News allies have aggressively promoted hydroxychloroquine as a potential cure, despite top infectious-disease expert Dr. Anthony Fauci and others urging caution and noting that there was not enough evidence of the drug’s efficacy.
The Times reports the president’s family trusts all have investments in a mutual fund whose largest holding is Sanofi, the manufacturer of Plaquenil, the brand-name version of hydroxychloroquine. Associates of the president, including Commerce Secretary Wilbur Ross, have also run funds that hold investments in the pharmaceutical firm.
https://redirect.viglink.com/
As the wise old Mexican peasant says at the end of “The Magnificent Seven”– “Only the pharmacists have won.”
My guess is that people healthy enough to bike or run outside, have very healthy lungs to begin with, and the virus cannot find weak and exposed cells. And a decent amount of Vitamin D limits bacterial infections, making the person even healthier. Many fewer outdoor enthusiasts will develop a severe set of symptoms. Its only an hypothesis, but it could be tested with some type of observations.
We’re talking about a virus, not a bacterium. Vitamin D does nothing that would affect a virus.
A person that exercises outdoors improves the health of their lungs enough to deprive the virus of infection sites, It could tested observationally, or in a lab to find the mechanism. People in Colorado are outside on the trails. But the infection rate is not climbing, so far. The chances of outdoor transmission among healthy people is being measured now.
This is mainly true. Having one chronic disease such a diabetes or hypertension doubles your risk of death from COVID. So yes, the usual advice of get off your ass and exercise and stop eating junk applies. I will give caution advising specific supplements or vitamins to protect from the virus. Try not to emulate our troll in chief with hydroxychloroquine.
While I know we’ve heard persons with certain co-morbidities are at higher risk, quantified risk varies.
If you have a citation you’re reading this specific number from, please provide it.
Potentially bogey data, real time reports here and may have to click through and scroll co-morbidity table. I leave it to the experts to quantify. It is being used now by the “so what people will die let’s go back to business as usual crowd”. My swag is that years of productive life are being taken away from the under 60 fatalities and then survivor side effects and fetal effects real time experiment.
https://covid19tracker.health.ny.gov/views/NYS-COVID19-Tracker/NYSDOHCOVID-19Tracker-Fatalities?%3Aembed=yes&%3Atoolbar=no&%3Atabs=n
Yes, correct, I did not mean to use the word double as a statistical term but as an approximation. Different co-morbidities vary. But the data does show surprisingly high numbers.
I think we will see a trend toward higher mortality with specific co-morbidities but there will be differences by country. This is why it’s important not to swag this number.
We’re seeing people attributing race to higher mortality in the U.S. but it’s a much bigger, deeper issue and the numbers are going to be important by location.
I will have to see the exposure methods correlations for cases before looking for race to be the first order correlation. Working in long term care facilities, Covid-19 hospitals, taking public transit, working in close quarters or getting the virus from someone doing any of the former. One critic is blogging around saying workers brought the virus to patients in LTCs. As many if not more staffers seem to be positive than patients. Maybe some have never thought about a staffer without PPE cleaning up after a patient or patient to patient exposure during cruise ship like communal dining.
The place my mother lived in – independent/assisted living – had four-to-a-table meals, and the tables were no bigger than card tables. Plus the rec room, and the lobby, where people liked to sit and talk. Elevator, because three floors.
I have only visited a handful of facilities. In two parts of the country the staff is predominantly POC as opposed to the patients. One sight burned into my mind is finding a distant relative lovingly, gently placed on sheets on the floor and leaning against the wall while his sheets and disposable bed pad were changed. Patients would more easily infect staff without PPE than passengers on a cruise ship infected their servers.
We are seeing marathoners and the like go down with this, though it’s a small minority. Honestly we just know so little about this bug it’s impossible to be sure. As for Vit D, it’s good for everyone all the time to not be deficient, and that does impact the immune system, but there’s little evidence having more than you need helps.
There will be a lot of data. It won’t be a controlled experiment, so it may have to be a county by county regression study. Something was different in the western states, but its probably more than one variable.
Population density, date of school shutdowns and other closures, average BMI, and smoking, may be involved.
Crap QN, I’m a runner and had high hopes…
However, I’m still going to claim (hope at least) that regular running will help. Covid-19 stresses the heart and the lungs as does running. But over time one’s body will adapt to the stresses of running and thus make it better able to cope with Covid-19 (again i hope).
Studies of the effects of aging on VO2 max suggest that my cardio-vascular system is statistically similar to someone 20-25 years younger than I am (I’m currently 67). As we know, Covid-19 deaths rates increase with advancing age. Also II recall reading that roughly 70% of Covid-19 deaths are accompanied with underlying conditions. Regular running (and intermittent fasting) also helps with metabolic disease and with hypertension.
I recently read “The Science of Running” by Steve Magness and found that I had been doing it all wrong. For Covid-19 benefits easy runs keeping your heart rate under 75-.80% of max is sufficient.
As you so eloquent suggest, sans vaccine we are all gonna get it. So let’s all take care of our health and go down swinging.
I suspect a lot of transmission occurs on surfaces, like door knobs, and faucets. Social distancing is working and we will know why pretty soon.
From the Boston Globe: “Massachusetts to launch first US trial of Japanese coronavirus drug”
Three Massachusetts hospitals have received approval to launch the first US clinical trial of a Japanese flu drug that could be used to treat COVID-19, according to one doctor involved in the effort.
The trial — which will take place at Massachusetts General Hospital, Brigham and Women’s Hospital, and UMass Memorial Medical Center in Worcester — was approved by the federal Food and Drug Administration Tuesday. The small, randomized trial of the Japanese antiviral drug favipiravir will look to study its effectiveness as a treatment for patients infected with the coronavirus, according to doctors involved in the study.
The Japanese government has touted the drug, known by the brand name Avigan, as a possible treatment for COVID-19
https://www.bostonglobe.com/2020/04/07/metro/massachusetts-launch-first-trial-japanese-covid-drug/
Does anyone here have information on how long the Covid-19 virus lives at various temperatures? I’ve done some looking, but don’t have confidence in the sources I found.
Apologies if I missed that info here.
A study was released March 27 — note that it’s a pre-print:
Study of aerosolized SARS-CoV-2 doesn’t not examine temperature but it does discuss viability of the virus on certain services within a temperature range.
My understanding is that at room temperature, it’s hours for paper and fabric to maybe three days for plastic and stainless steel.
I gave the study for that, PJ. It’s the aerosolized study. Once again:
Surface stability. That.
EDIT: Because a simple breakdown of the study appears necessary:
1) SARS-CoV-2 remained viable in aerosols throughout the duration of our experiment (3 hours);
2) (a) SARS-CoV-2 was more stable on plastic and stainless steel than on copper and cardboard;
(b) viable virus was detected up to 72 hours after application to plastic and stainless steel surfaces;
(c) activity of virus dropping more quickly on stainless steel than on plastic;
3) On copper, no viable SARS-CoV-2 was measured after 4 hours;
4) On cardboard, no viable SARS-CoV-2 was measured after 24 hours.
Shorter answer, for people who don’t want to read studies. (I can, but it’s a PITA.)
For those who don’t want to read entire studies I would suggest at least looking at the abstracts. Abstracts are at most a paragraph or two and provide a summary of the paper.
Unless I’m a domain expert I rarely find it useful to read entire papers; I just don’t understand nuances in the information.
In this particular case it was a seven-paragraph letter at the link provided without an abstract.
Right. Just what we need is more TL;DR.
Then lift the key parts from the study or abstract or don’t comment. “My understanding” is like “I heard” when there’s no citation to support it.
I do read some – but it’s hard going even when it’s a field where you know something but not a lot.
Hey thanks for posting these, I meant to link the one and then forgot when I was getting this up later than I meant to.. I’m going to go back and putting in links now.
Quinn, thank you very much for this excellent article which I will forward to the few people who listen to me:)
I had intended to comment your FAQ post(s) but comments had already been closed.
If not for your warning, I just might have licked a pangolin if I had met one, but:
https://www.bbc.com/news/science-environment-52048195
So the Nature Medicine article on the origin of SARS-CoV-2 has a nice figure (figure 1) that schematically represents the similarities and differences of the Spike protein among different bat, human and pangolin coronaviruses.
The upshot is that while overall, SARS-CoV-2 is most genetically similar to Ra-TG13, a bat coronavirus (something like 96-98% identity in the genetic and amino acid sequences of the proteins), where it differs substantially is in 6 key amino acids in the receptor binding domain, the part of the protein that binds to cellular ACE2 (the cellular lock, if you will).
Those 6 amino acids are L F Q S N Y from amino to carboxy end in SARS-CoV-2. The same 6 amino acids in SARS-CoV-1 are Y L N D T Y (only the Y is conserved). In Ra-TG13 (the bat coronavirus very similar to SARS-CoV-2), the same 6 amino acids are L L Y R D H, so just the L is conserved. For technical reasons that I’m not going to go into here, the SARS-CoV-1 sequence is actually a much better fit for the SARS-CoV-2 sequence than the Ra-TG13 sequence, even though there is more overall genetic similarity in other areas between SARS-CoV-2 and Ra-TG13. Not surprisingly, both SARS-CoV’s Spike protein bind human ACE2 well, (CoV-2 binds much better than CoV-1), and RaTG13 which has more amino acid diversity in those areas, not surprisingly, does not bind ACE2 at all, which makes sense, because it’s a BAT virus.
Intriguingly, the pangolin coronavirus on the other hand, has *the exact same* amino acid sequence at those 6 key spots as does SARS-CoV-2. I haven’t seen data regarding what the pangolin S protein binding to human ACE2 is, but I wouldn’t be shocked if it’s better than SARS-CoV-1. A recent paper in Nature also compares several pangolin coronavirus isolates from various trafficked animals in China, and finds overall 85.5% to 92.4% sequence similarity (I think at the genome level) to SARS-CoV-2, which is very close, but still bat RaTG13 is a better fit. However, this indicates that SARS-CoV-2 may share some features of both, notably most of replication machinery and virulence factor proteins from RaTG13, but obviously much more of the receptor binding domain similarity from the pangolin virus. So it’s possible that maybe it arose as a recombinant of the bat and pangolin virus, although that same Nature paper also posits it could be “convergent evolution” of the receptor binding domain in some SARS-CoV-2 ancestor that was circulating in bats before making the jump to humans.
I might note that the Nature paper also points out that pangolins as an intermediate host seem an unlikely choice given that they are critically endangered in the wild and are solitary species, which I would agree with. So the mystery of the virus’ origin still remains unsolved.
Millions of pangolins have been smuggled to China and other Asian countries over the past few years. https://www.nationalgeographic.com/magazine/2019/06/pangolins-poached-for-scales-used-in-chinese-medicine/
So with that trade going on to wet markets in China and elsewhere, not such a mystery how they could have gotten involved.
I believe pangolins are used in Chinese medicine;
but whether a virus could survive the usual preparation is an open question.
https://www.nature.com/articles/141072b0
http://www.chineseherbshealing.com/pangolin-chuan-shan-jia/
Ah, but it still is. SARS-CoV-2 is a BAT Coronavirus in the main. How would a BAT Coronavirus get into a Pangolin at a wet market, where the Pangolin may already be dead? Would live bats and pangolins mingle together? And for how long? It takes time, probably on the order of months at least for a cross-species virus to adapt to its new host. Would the bats and pangolins be together that long?
My point is that in nature, these 2 animals are never together. If SARS-CoV-2 is a recombinant virus, as some have postulated, how long could the Pangolin have had it before it was slaughtered?
Make no mistake: I believe that the RBD domain of SARS-COV-2 Spike is likely of pangolin origin. Question is, how did it get there, when the rest of the virus is clearly of bat origin?
Perhaps humans were the true intermediate hosts… Or maybe domestic animals? There’s evidence that SARS-CoV-2 can somewhat infect cats and dogs…
Presumably the intermingling between pangolins and bats was from commercial farming of pangolins?
I think we’ve seen another example this week of the ease with which SARS-CoV-2 infects cats.
Thanks for explaining why this ugly little critter actually thrives via its nasty little stickers.
I found an article about various neurological manifestations of covid19, sometimes appearing before “typical” ones.
https://www.lemonde.fr/blog/realitesbiomedicales/2020/04/07/covid-19-les-symptomes-peuvent-etre-neurologiques/
If the French scares you, jump to the end for the references:)
Thanks for sharing that. It’s the rare article appearing in a large news outlet — regardless of country — which is *extremely* well sourced with an amazing amount of citation. (Anybody wanting to read it who isn’t proficient in French, try opening the link in Chrome and allow the browser to translate to English. You’ll get about 98% comprehension with this piece, in spite of the technical terms.)
I think, though, that this is a rare case; SARS-CoV-2 attacks ACE2 receptors and brain tissue has relatively few out of all body tissue. Breaching the blood-brain barrier is also a leap the virus would have to make first before attacking the brain’s few receptors. But for the few people in whom this leap is made? Awful — doctors clearly didn’t know what they were up against.
I’m also amazed I haven’t already heard about this particular case since the patient was treated in Detroit. Could be that the study was in a radiology journal, not usually the first in which you’d expect to see news related to a viral pandemic.
EDIT: Two things —
1) The subject of the study was an airline steward treated in Detroit. This is important to note; are some asymptomatic carriers not really asymptomatic, but having symptoms which don’t fit the criteria like a headache and nothing else? Do airplanes factor into this because of pressurized cabins?
2) The number of ACE2 receptors across different human tissue was measured in a Chinese study. The lungs and small intestine contain the highest number of receptors. See:
I saw a news story about some people having neurological problems with the virus.
https://www.sfgate.com/news/article/Some-Coronavirus-Patients-Show-Signs-of-Brain-15172979.php
NEW:
With ventilators running out, doctors say the machines are overused for Covid-19
https://www.statnews.com/2020/04/08/doctors-say-ventilators-overused-for-covid-19/ APRIL 8, 2020
Remember back when we were talking about this?:
Exclusive: Pressed by Trump, U.S. pushed unproven coronavirus treatment guidance
https://www.reuters.com/article/us-health-coronavirus-usa-guidance-exclu/exclusive-pressed-by-trump-u-s-pushed-unproven-coronavirus-treatment-guidance-idUSKBN21M0R2
APRIL 4, 2020 / 1:52 PM
Well, yesterday evening, Reuters wrote:
CDC removes unusual guidance to doctors about drug favored by Trump
https://reuters.com/article/us-health-coronavirus-usa-cdcguidance-idUSKBN21P39R
APRIL 7, 2020 / 5:04 PM
This was our conversation about the original article:
https://www.emptywheel.net/2020/04/07/like-all-else-trumps-inspector-general-turnover-is-about-pandemic/#comment-836549
Here’s the new guidance:
Information for Clinicians on Therapeutic Options for Patients with COVID-19
https://www.cdc.gov/coronavirus/2019-ncov/hcp/therapeutic-options.html
Updated April 7, 2020
Good. Quite a few doctors have come out and said hydroxychloroquine was problematic, including Swedish and French.
https://www.acc.org/latest-in-cardiology/articles/2020/03/27/14/00/ventricular-arrhythmia-risk-due-to-hydroxychloroquine-azithromycin-treatment-for-covid-19
https://www.kptv.com/news/ohsu-cardiologist-raises-concerns-about-drug-linked-to-covid-19-treatment/article_ee2d0e66-760d-11ea-a590-53bbefb20427.html
With the damage SARS-CoV-2 does to hearts, hydroxychloroquine was too much additional risk.
NOVEMBER:
Intelligence report warned of coronavirus crisis as early as November: Sources “Analysts concluded it could be a cataclysmic event,” a source says. https://abcnews.go.com/Politics/intelligence-report-warned-coronavirus-crisis-early-november-sources/story?id=70031273
April 8, 2020, 4:01 AM
related: Some researchers think the virus might have gotten to California last fall.
https://www.sfgate.com/bayarea/article/Study-investigates-if-COVID-19-came-to-Calif-in-15187085.php
(I was hearing stories from people in January about a bad flu that just kept holding on.)
Well, I can’t keep up, obviously…Marcy wrote about this in a new post today:
https://www.emptywheel.net/2020/04/08/the-very-specific-details-about-the-warnings-from-the-deep-state/
[Thanks for the info, PJ Evans!]
I am having a hard time understanding the terms peak and surge. When government health officials use these terms are they talking about total cases? cases requiring hospitalization? deaths?
As I already wrote, I’m just an IT guy whose only contact with medicine was an 18 month stint in a clinical (blood bank) lab. This might be something for the specialists here.
https://www.biorxiv.org/content/10.1101/2020.03.12.988865v2
“The architecture of SARS-CoV-2 transcriptome”
not peer reviewed yet so take with salt
While searching for the research behind
https://www.yna.co.kr/view/AKR20200408113400009?section=safe/news
sadly enough I didn’t find the mentioned EMBO journal article, yet, but two mentions of TMPRSS2:
https://www.eurekalert.org/pub_releases/2020-03/dpp-pso030520.php
https://www.eurekalert.org/pub_releases/2020-03/tiom-nie032420.php
ha, found:
https://www.eurekalert.org/pub_releases/2020-04/bifg-wcd040720.php
Quinn Norton you are amazing! the article made me laugh and provided informaiton which I was able to understand. If I read it a second time I may even be able to explain it to others. this is how science ought o be written, you know for those of us in the english or hisory dep.t.
The line about who god may have love most is a riot.
thank you for writing this article. make me laugh and provided information.
p.s. the care worker set up my lap top so I’m no longer relient on the cell phone. however, I can’t always see what I’m writing, I touch type, so please forgive my errors or don’t make sense.
\o/
I’m glad it’s useful to you!
This is a summary of information on home-made masks.
https://www.sciencenews.org/article/covid-19-can-fabric-cloth-masks-stem-coronavirus-spread
Info is just all over the place:
3-19-20 on twitter:
C. Michael Gibson MD
@CMichaelGibson
Cambridge scientists tested 0.02 micron Bacteriophage
MS2 particles (5 times smaller than the coronavirus) &
compared homemade masks made of different
materials to surgical masks.
Surgical mask blocks 89%
Vacuum cleaning bag 85%
Dish Towel 73%
T shirt 70%
Then there’s a more in-depth (and pessimistic re effectiveness, to some extent) analysis with a bunch of graphics and variations such as doubling the mask material here:
ht tps://smartairfilters.com/en/blog/best-materials-make-diy-face-mask-virus/
I *had* to go to the post office today and so wore a mask for the 1st time. South suburbs of Chi, the PO employees all masked and the joint stinking of Lysol, about 7 of 10 of the customers were masked, but 6′ distance was observed except upon entering or exiting where people just went through doorways without heed. Glass doors, you couldn’t see me coming?
Speaking of CCR5, this little company CytoDyn Inc (CYDY) seemed to just address that problem with a press release today.
https://www.cytodyn.com/investors/news-events/press-releases/detail/413/blood-samples-at-day-0-3-and-7-for-severely-ill-covid-19
I don’t own the stock.
Just hoping it really works for our sake.