![[Photo by Piron Guillaume via Unsplash]](https://www.emptywheel.net/wp-content/uploads/2017/07/Healthcare_PironGuillaume-Unsplash_v1-1030x687.jpg)
Vertical Demand Curve: When Your Money or Your Life Isn’t a Choice
[NB: Byline — check it. /~Rayne]
Hold this thought: depicted above is a gun.
Like nearly every freshman student, I took my Economics 101 along with Intro to Business, Accounting 101, Intro to Marketing my first year of B-school.
This is when the indoctrination begins, when these squeaky-new eager beavers departing their teens are slowly steeped in the toxins of American-style business.
I was an older than average student, though, having switched majors after working for a few years before I returned to school. I’d seen and done things before I returned to the classroom, squinting often at a blackboard in disbelief.
My first econ prof was fairly young himself; he was also an avowed libertarian. Everything he taught was colored with the perspective that government was a bad thing. My younger cohort went along without questioning this view.
And yet our prof had a difficult time saying government was bad when introducing us to supply and demand curves.
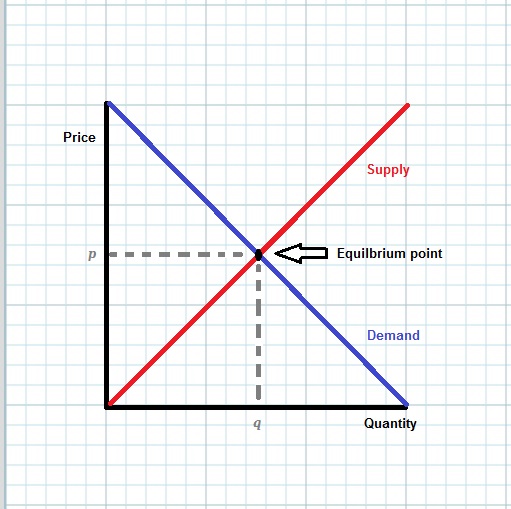
More supply, price goes down. More demand, price goes up. The degree to which the market is sensitive to price or demand is reflected in elasticity. Basic.
But then we were presented with the vertical demand curve — when the buyer will pay anything for the available supply, when demand is perfectly inelastic.
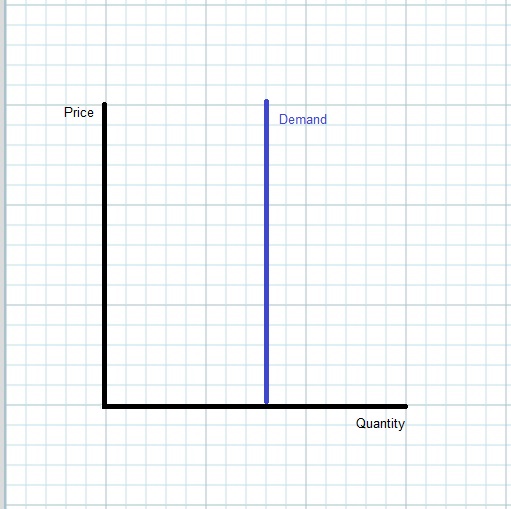
This is the model for business in which the supplier demands your money or your life, a gun to one’s head, “Give me all your money or you’re dead,” a perfectly inelastic demand curve.
Libertarian prof called this extortion. The dutiful 18- and 19-year-olds in class nodded their heads, fighting a yawn. From the look of them none had experienced this caliber of threat.
Prof made a departure from “government is bad,” by insisting this is the point when government should regulate the market. He said it was illegal to base an exchange on forfeiting every claim to rights including one’s life; we prohibit extortion.
This is why health care should be regulated, he said. I was a little skeptical at the time; this was smack in the middle of the Reagan years and there wasn’t a lot of regulation on health care per se. If you got cancer there weren’t many options no matter how much money you had; doctors cut it out or tried to zap it with a limited range of therapies.
The risk then wasn’t the cost as much as the gamble of effectiveness. I lost a dear friend to the after-effects of available therapy; they survived a bone marrow transplant in the early 1980s but their immune system failed.
Decades later we have a sizable number of therapies for illnesses which are effective and keep people alive, but the number of people who suffer from some of these illnesses are so low that these drugs aren’t profitable. The Food and Drug Administration has helped in these cases — until now.
The “gun” in the image above is a money-or-your-life situation for patients with Lambert-Eaton Myasthenic Syndrome (LEMS), who may require permanent hospitalization or suffocate and die without this drug called Firdapse.
Thanks to the FDA calling Firdapse an “orphan drug,” the company which owns its intellectual property rights will now charge $375,000 a year for this medication.
One patient in Iowa said she’s willing to pay something for the medication but a year’s therapy is three times what her house is worth. She doesn’t know if her health care insurance will cover it.
This isn’t even your money or your life now — she doesn’t have the money.
She’s gotten the business end of the gun without any warning, after having benefited from the drug for years.
This is worse than extortion; it’s a death sentence for anyone who isn’t a billionaire. Yes, billionaire because someone worth a million can pay for a little more than two years of this drug and that’s it.
Why Catalyst, the company which owns Firdapse’s intellectual property, even bothered to buy this drug is beyond me. If the three million patients who currently rely on this drug can’t afford it, there’s no profit to be made, no recouping the cost expended to buy the rights to the drug.
With only a couple thousand billionaires in the world I find it hard to believe enough of them will develop LEMS and pay for Firdapse to make the acquisition worthwhile.
It’s not just an unethical business, creating a gun to hold and fire against the heads of LEMS patients.
It’s really stupid business to aim an economic gun at one’s self.
I wonder all these years later how many former B-school students struggle with the vertical demand curve lessons once they enter the real world.
And I wonder what the supply curve looks like when it comes to insulin, the price of which has jumped dramatically over the last few years so that it has become your-money-or-your-life proposition for many diabetics.
At what point is insulin no longer profitable — after 10, 25, or 50% of insulin-dependent patients die because they can’t afford it, is it no longer profitable to make insulin?
Treat this as an open thread.



Hey, I freely admit I am NOT an economist. The vertical demand curve really ends when the patient dies/runs out of resources/both.
Be nice to bmaz because I have to run an errand and can’t be here to take a beating about this economics+health care post.
WARNING: Any comment offering medical advice will be tossed in the bin.
Do NOT tell anyone what to do about their diabetes. Anyone with a chronic health problem should consult their licensed physician.
It is much the same for asthma/COPD inhalers, which can run 200-400 dollar apiece. And I do so like to breathe.
Now this is something I know intimately about. Been using them forever. Used to be dirt cheap relatively speaking. They did skyrocket in price. They can be had more reasonably again though. I get mine for about $25 a piece now through insurance. But there are other deals out there like through GoodRx. It is still stupid though. You can buy a package of three inhalers in Mexico or Canada for about $9. And they work about the same.
the computer at my doctor’s office has a persistent tendency to change my birthdate to that of the friend who got me in there the first time, back around 2011 – and that puts me under 65, so they try to charge full rate for the generics I take. One of them is like $160 for three months, instead of the $25 or 30 that I pay under Medicare. It’s a standard blood-pressure medication. One of my blood-sugar drugs is $900 for three months – I hope that’s for the brand name – and it’s $18 otherwise; the other is $63 vs $12. The statin – again, a standard drug – is $800 vs $22.
They could make as much money with reasonable prices, maybe even more, if people could afford the drugs they need, instead of skimping on them or doing without.
What is sick is that they do that with common everyday stuff. Albuterol, blood pressure meds, and maybe the most egregious right now, common insulin.
All of mine are generics, nearly all are common, standard drugs for the medical problem, and there’s no reason any of them should cost that much: they’re not biologicals, and they’re not something like monoclonal antibodies that are more difficult to make, even with bacteria/yeasts doing all the actual work; they’re simple pills that are drugs that have been around, in some case for decades.
Yep. But years ago, I used to buy vials of common human insulin, but for my diabetic dog, because it was cheaper than veterinarian insulin. My vet told me to do so. A month’s supply, including the box of syringes, was like $40. A month’s supply of insulin is now somewhere around $400. That is just stupid profiteering.
You’re correct. I do wonder what the companies buying orphaned – and other – drugs are even trying to do, when they price themselves out of the market.
Personally, I favor regulation along the lines of that for utility companies: they can make a reasonable profit (for utilities, it’s something like 10% max), but they must justify their charges – every year.
Of course, then they take the route of buying a majority of the regulating commission – which works up until they do something egregious, like starting a major fire or blowing up people while trying to game regulations [*ahem* PG&E *ahem*]….
[I’m lucky – my treatment is covered by Medicare, though I still have to pay a share of it – but I won’t go broke doing it as I have some investments (mostly inherited), and the long-term drug treatment currently runs less than $15 a month. It’s a good thing that what I had responded well to chemo – a lot don’t, still. But if I get it again, which is possible though more likely to be Some Other Kind, I’m opting out.]
Arguably the problem here is the government granting monopoly rights to produce the drug.
Accurate assessment.
I work in healthcare. We constantly debate cost benefit analyses.
These Pharm companies seem to struggle with the concept.
Much like the right does, the short term benefits always trump (pun sort of intended) any semblance of long term sustainability.
To be honest? It’s effing insane how short sighted these people are. And in the most damaging and heartless manner imaginable. It’s truly horrific.
Hi Mookieb, and welcome to Emptywheel. Come join us often in comments, and you are right that the pharma scene is freaking insane.
Also…pricing is not transparent. All those nice graphs you see about market efficiency and supply and demand assume that people can shop around, know what they are getting, and know what they are going to pay. None of that is true in healthcare.
Some of the health claims people sat across from my department at “medium sized insurance company”. They had a claim that came through the Mayo Clinic, and ended up costing 1.4 million. We offered 140k and the offer was accepted.
So the cost of drugs/healthcare that you see being charged, is not necessarily what is getting paid.
Another reason the market is inefficient and needs much better regulation.
That, the lack of transparency. All the anti-government/free market guys reject single payer as socialized medicine but it already ~is~ socialized in favor of businesses by allowing them excessive opacity in operations.
Not a pharma expense, but hospital billing:
My son was referred for a brain-stem MRI b/c his QEEG suggested a TBI in early childhood. Went to Children’s Hospital: sticker price $5,672. In-network insurance paid $334.90. Children’s accepted that (with $25 copay). I know — we’re so fortunate to have insurance. It’s still Unbelievable.
It’s absolutely ridiculous. It’s a big magnetic camera and they’re charging nearly 6K for a could of snapshots?
It’s this kind of thing that makes me think about going overseas for medical tourism. I have one friend with a heart problem who moved to Thailand because it was so much cheaper there for their fairly basic care.
It’s a big expensive piece of equipment. Which they want to keep busy, but they also have to pay for it and the parts and the specialists who maintain it. (The similar one that they use for radiation broke and took two days to get fixed. First time I’ve had an actual medical appt on a Sunday. It’s like the CT/PET machines, a doughnut that they roll the bed in and out of, and it actually does do imaging – they do a test image before nuking you.)
I know it’s expensive equipment BUT they aren’t new technology and these machines are used around the world, not just here. So why do any imaging orders cost thousands of dollars here when they cost hundreds abroad?
Only thing I can figure is this is a guaranteed money maker they can rake a lot of money in with to allow room for negotiation on other more variable services.
Also, that fancy picture? The kid has to be held perfectly still, which usually means deep sedation (in a kid you’re worried about TBI, no less) which means a well trained and expensive anesthesiologist using a no-metal sedation setup (because giant magnets cooled with liquid helium). Also, do you want those pictures to go or are you going to eat them here? I’m assuming you’d like a well trained and expensive pediatric neuroradiologist to read the images and tell you what they actually mean.
There’s a lot that goes into that glib ‘couple of snapshots with a magnet’ comment. MRIs are close to miracles.
Even for an adult, scans aren’t easy. The PET scan took half an hour, maybe more, and you can’t move more than you need to do to keep breathing. (I was lying down with my arms extended – my shoulders were Not Happy. Also doing it fasting…) The CT scan is faster, but you get to hold your breath almost too long (it’s got the computer telling you when to breathe). For a kid, it would be much harder.
Your pet scan looked at positrons…its using frikin’ antimatter.
Don’t get me wrong, there are huge issues with the way medical care is billed and paid for in this country that could be solved in a less expensive and more socially just way. But there is a lot of technologically challenging care going on that is going to be expensive. We’re talking about liquid helium and antimatter here. Not to mention the people that keep you safe during the study, make sure the study gets the information you want, and interpret the results. Those humans are well trained and expensive.
It’s the still same technology used overseas — hell, across the northern and southern borders by mere feet and miles — no matter how advanced it is. I’m not going to be put off by the ooga-booga-oooh-high-tech! talk; we’re carrying pocket-sized devices with multiple times the amount of computing power the Apollo 11 mission used when it landed on the moon.
But I have actual competition for the device in my pocket. I pay a price for it comparable to what I’d pay for it overseas. Somehow that breaks down when it comes to the application of medical technology in U.S.
Ugh. I should also point out here I have multiple health care professionals AND engineers in the family, including a biomedical engineer (and another one in college who may yet go for their PhD). Medical technology is what they use and what they design and manufacture. They know there’s a massive scam going on. I dread calls from my mother who has +50 years health care experience telling me about the latest fuck-up she or my dad has experienced — like ordering unnecessary tests and scans every single damned time they show up.
If you think a test is not needed, then don’t get it done. Doctors suggest diagnostic and treatment plans, they (in general) don’t force you to do them. Adults can make independent choices and live with the savings, and consequences, of those choices.
I’m just trying to point out that there are things you are ignoring that are legitimate costs associated with imaging beyond a few seconds for a ‘snapshot’, as you put it. In the case listed, $334.90 for an MRI that probably had sedation and a radiologist to read it seems a pretty good deal to me.
If my parents didn’t have health care backgrounds they wouldn’t know enough to realize they didn’t need another bloody scan they just had 6-12 months ago.
The average American patient suffers from white coat syndrome — they believe all too easily what they’re told by someone in a white coat. It doesn’t help matters when they’re told, Oh, this is really complicated stuff! So technical!
On the other hand, I laid my body down, sat perfectly still, was in and out of the device in less than five minutes. No one touched me the entire time.
However I waited *alone* in a waiting room with +100 empty seats for an hour for this five minute snapshot while the administrative folks tried to figure out how they lost my appointment AGAIN, twice in 10 days time. I saw more administrative people than actual health care providers.
I don’t mind being billed for the extra labor it takes to care for a neonate in distress. By all means, be sure to break out what the actual expenses were for such care in a generic fashion so the public can see it.
I do mind being fucked over and not being told, Oh, by the way, all this extra time, effort, and resources when we didn’t actually render medical attention pays for the neonate down the hall.
I’m still goddamned pissed off about that two-acre waiting area under air conditioning in which nobody ever waited with me.
I’m not sure why you’re trivializing medical scans by calling them ‘snapshots’. I’m agreeing with you that medical billing is byzantine and opaque, and that administrators can spread like measles in Portland, and I’m sorry you had to wait for the study. But if it was a medically needed imaging, it really wasn’t a ‘snapshot’.
They’re snapshots. You’re intimidated by terms like “antimatter” when MRI/CT/PET devices do what the earliest photographic plates did: capture energy emitted in a manner which forms a representation of the object around/ through/from which electromagnetic energy has been emitted.
Now instead of chemically-treated plates behind a lens we’re talking a half-million to $2 million camera.
Look, I can see you’ve been frustrated by medical care for a lot of reasons. You’re conflating problems with the way medicine is billed and paid for (which are two tremendously different things) with a long list of grievances you have with US medical care that extend far beyond that. Your ‘snapshot’ response to a medical scan shows you don’t value the care being given and the expertise that is involved in interpreting it.
I don’t understand why, if you’re so dissatisfied with medical care and think that its just a snapshot or two, you don’t just disengage from the system? If it isn’t helping and its such a trivial thing don’t get it.
I could list the things that medicine has done that would have been considered miracles just a decade or 2 ago. Cystic Fibrosis was a death sentence in the 80’s, and with the CFTR modulators now most can expect to live a normal life (if they have the right mutations).
When I was a stupid kid in the 80’s I got hit by a car, they did a CT to see if there was a bleed. It was 64×64 pixels. You could barely tell there was a head there to scan. Now they’re doing 2048×2048 with sub-MM cuts…MRA and functional MRI…all amazing ways of getting data.
Expensive ways to get data. That needs an expensive person to interpret it in your clinical context.
In our area, there’s been significant medical consolidation as the medical school hospital has gobbled up a lot of independent surrounding facilities. So far, it’s been a net benefit: they have a single schedule for all of the expensive scanners, and put people in wherever the next available appointment is.
year before last, I got a mammogram, an ultrasound, a biopsy, a CT scan, a PET scan, and, a couple of weeks later, an echocardiogram. The CT/PET scans were billed at $9200 – without the radioactive agents. Medicare approved about $2400, and my share was about $500. I doubt that the (very busy) imaging place is losing money. The echocardiogram – I paid about $100.
Chemo was billed at nearly 18K per session. I get to pay about $1800. (There were five of those; the first one was about double that, but they used more drugs. And actual needles, because the port went in the next day. That’s another $600 on my bill.)
Medicare tells me what they were charged, what they approved, what they actually paid, and what they think I’ll have to pay. The difference between what they were charged and what they approved is big – and so is the one between approved and paid.
Kaiser did a huge study a few years back of how the orphan drug system is being abused for profit. Pharmcos will take a drug that already has mass-market FDA approval and then test it on a small (even tiny) ‘disease’ subgroup and get an orphan designation for that group (of the same drug that is already on the market). For some drugs, they do this over and over- called ‘salami slicing’- so that the seven years’ exclusivity gets extended over and over, even if the original patent has fallen out. They also get gov grants and other benefits out of the orphan drug application process, besides driving up costs to people who need the drugs. This is common with cancer drugs and those for autoimmune-type diseases; also at least one of the cholesterol drugs.
Below is an overview of the problems, with additional links in the sidebar. It’s worth reading because: (1) it’s way worse than what I summarized– see the quotes by the former FDA guy who now has a business helping companies do all this (one snippet quoted below); (2) there will likely be some legislative moves against this, and the issue is complicated because talking head pros cite examples of _actual_ orphan drugs and stuff like ~’we don’t want dead children’ to try to argue against any changes to orphan drug regs.
Drugmakers Manipulate Orphan Drug Rules To Create Prized Monopolies | Kaiser Health News
Oh, plus my guess as to the ‘money-or-your-life’-type pricing is that it’s an attempt to move the Medicare payor Overton Window. What Medicare decides to pay, private insurers tend to follow (not always, but it tends to NOT go the other way around: i.e. gov decides what gets paid first). …perhaps combined with some ‘parking effect’- i.e. the gambit could be to sit on the orphan status benefits, see if Medicare et al. budge on reimbursements while the seven-year clock runs… If it works out for them, they can maybe cut another salami slice before the deadline, or move onto another product/disease category and try the same thing. (i.e. it’s no coincidence that common, essential drugs like insulin are among the price-movers.)
I was taking one of those orphan drugs, Imbruvica (Washington Post did an article about this), which would have been at least $40,000 a month if I’d paid out of pocket (more now), but because I didn’t have Medicare Part D (luckily, because I couldn’t pay %20 of $40,000 a month either), the drug company gave it to me free as long as I continued to have too little income. I was grateful (until sudden side effects made me unwilling to touch it again), but could not get over the insanity of the pricing, and the fact that they could get away with it.
Imbruvica used to be cheap as dirt, so the company hadn’t been trying to recoup any R&D costs for some time, but when they found a new use, and because Medicare didn’t fight it (most patients are over 60), the price smashed through the roof. My doctor said Medicare administrators could have refused to pay for anyone to take it and forced the price back down, but we apparently don’t have proactive administrators in those positions.
Libertarian or no, most people surely agree that viciously predatory pricing ought to be opposed. Vitiate the agreements that let companies go back to charging fatal prices for HIV drugs in Africa after the current lull, let us all buy from whatever country produces alternatives to our lifesaving (or otherwise necessary) drugs, and figure out a formula for how much anyone can charge for something the government funded the research for. The current strategy is outrageous and baffling and seems to have been developed by aliens trying to destroy us.
…developed by aliens trying to destroy us.
The call is coming from inside the house, yes? ~smh~
I’ve avoided looking at the cost of the inhaler I needed for a short period of time. I’ve been afraid the shock would cause shortness of breath and I’d need the damned thing again.
I’m an oncologist, and the strategy you describe, where the drug company pays the cost of highcostium, or pays the 20% due in the Medicare Part D plan if your income is low enough, is crazy-making. What they do is blunt public outrage about the price of the drugs because, after all, you’re getting it–while they still get the overpriced 80%. And this doesn’t even take into account the fact that many of these drugs come from initial research in labs funded by government grants, in other words, your tax money and mine.
Thanks for your feedback. We really need more transparency about the amount of public investment in pharma research and why we are paying multiple times over for drugs. Welcome to emptywheel.
All those simple charts have little or no relation to people or how they act. Economics it must be understood doesn’t have anything to do with people.
Sorry to interrupt and go all meta but not doing so dooms you and us and everyone. Fighting about demand curves leaves one fighting in their ring and you will lose.
Demand, supply and prices cannot be discussed without discussing how the market is organized.
Go here and jump to the 11 minute point. Then watch the whole thing.
https://www.youtube.com/watch?v=xfbVPDNl7V4
Meh. Markets are far more complex than the simple models we learn in Econ 101. As Doc Searls and David Weinberger explained it in The Cluetrain Manifesto, markets are conversations. You’ve spent enough time here to use this place as an example of a highly complex conversation. Sometimes markets are made deliberately fuzzy to prevent oversight, to prevent unwanted participants in the conversation between producers and money.
But one demand curve is my primary concern and it’s both the simplest and the deadliest.
When demand is vertical that’s when we must take collective action. Very simple.
The thing that gets me crazy about supposed free market in health care has to do with another aspect of econ 101.
Consumers are supposed to have information about prices so that they can seek the equilibrium point, choose substitutes, all of that good stuff. But that kind of information transparency is not an option for almost all of the expensive critical care that drives health care costs in this country, especially on the demand side but also very often on the supply side.
I’ve had family members go through several surgeries in the past decade, and consumers can’t make informed choices based on costs even if they could judge what procedures are needed. Doctors often can’t know what real costs are since they only bill for a piece of the care, and care is so fragmented that typically no one is really in charge of all aspects of hospital care. Insurers play catch up and make arbitrary decisions about reimbursement based on haphazard information as well. And in the middle of an ER visit, there is simply no time to evaluate costs even if anyone wanted to.
And this is true for many medications as well. If your doctor prescribes Highcostium, it is regularly the case that the patient is in no position to know whether there are more affordable options. And while sometimes the failure to prescribe a lower cost alternative is the doctor’s fault, other times doctors aren’t in a position to fully evaluate a case and know if a cheaper treatment will be equally effective. Patients follow advice they can’t evaluate, get locked into a treatment plan they can’t afford, and then lose the savings needed to pay for a plan they could have originally afforded.
Almost all libertarian and right wing economists are in denial about the information failures in modern health care, and yet try to pin the blame on consumers.
I took Econ 101 as an older student last semester. Luckily, my teacher wasn’t a libertarian, and he wasn’t shy about the need for taxation for public investment/a safety net. Someone walked out when he broke down the reality of supply-side economics(it’s a conservative area).
When pharmaceutical companies do things like this, it makes people suspicious of the medical field as a whole. As a result, people become fearful of doctors.
I don’t understand why politicians can’t say profiteering off of sick people is immoral. I think the public would support that.
I have some friends who sold everything and for the last 7 years just travel the world. Wonderful couple with 4 suitcases who blog their adventures (see “my” website – it’s there’s). They are in South Africa now. Jess is in the hospital tonight and tomorrow will have a triple bypass. Unsure if their UK health insurance company will get payment there on time, they had to scramble to come up with the cash or wait. $52,000 USD or . . . what, maybe a script for nitroglycerin?
That’s a gun to your head.
Yep, that certainly is an accurate demonstration of the vertical demand curve. Not much different here in the U.S.; if you don’t have coverage they’ll stabilize you — maybe — and then dump you.
The thing about a *market* is that it is a simplified model, with all the limitations thereof.
It *assumes* no friction, perfect information, and fungible sellers and buyers without significant individual power in the market behaving in an optimal economic fashion.
None of these apply to medicine…*especially* without some help from the gubmn’t. I am for a little government as possible, but…I am against extortion, especially with gubmn’t sanctioned monopolies called patents and FDA approvals!
Oh, honey, you sweet, sweet summer child: it’s not the patents and the FDA approvals that are the actual problem. It’s the corps that hold the patents and misuse them and the approval process.
I’m not entirely convinced that captures the problem.
The same pharmaceutical companies manage to supply drugs to other countries at far more reasonable prices. While you can argue there’s perhaps something if a free rider effect, it’s also likely the real problem lies with the structure of the entire US healthcare system.
And even if drugs were free, they represent only around a tenth of US healthcare costs.
Insurance companies that are for-profit (some have extremely-well-paid executives, and own hospitals besides), hospitals that are for-profit, drugstore chains that make enough that one is trying to buy an insurance company, clinics that are for-profit (dialysis and weight-treatment, mostly, I think), and, and the bottom end, specialists who enjoy their mid-6-figure yearly income and can’t live on only $200 or 300K per year. (And then there are the church-run hospitals that forbid standard medical procedures, even when they’re needed, because their religious beliefs override medical ethics. That needs to be fixed NOW.)
I’d like something like the system in Canada or the UK (before the conservatives started trying to kill it), but getting there is probably impossible. Maybe we could get something like the one in France or Germany, where the insurance companies exist but are very restricted by comparison with what they can do now.
The Mexican health care model is worth a look as well. It’s a hybrid, with a multi tiered public system operating next to a robust private market. There are some lingering structural issues related to the public sector part of the system, but those are being addressed now with the new administration. It’s by no means a perfect system (nothing ever will be of course), but for most of the country it functions very well.
The barbaric US healthcare industry is one of the reasons we no longer live there.
Good stuff.
I first came to health care analytics in 1993, hospitalization outcomes analyst and InfoTech guy with the Nevada – Utah Medicare QIO. A quarter century later we’re still chewing over the same stuff. I blog about these issues in some detail at KHIT.org. Did my first grad school paper in 1994 on the “Single Payer” proposal.
http://www.bgladd.com/PDF/JAMA1994SinglePayerProposalAssessment.pdf
Too much money on the table.
@Pat McClure February 11, 2019 at 9:57 pm
There’s also more than a little evidence of price fixing by corps of generics – they’ll pay other corps not to make or sell the generic.
And Medicare is blocked, by law, from negotiating prices – they’d do it if they were allowed. Just like re-importation of drugs is blocked by law, and all those cheaper-but-identical drugs in Canada or Mexico can’t legally be imported. (At least, not more than you can use in three months. And you better have the prescription.)
I am not as articulate as you, Rayne, and I do not have a theory of the case how we came to be (and insist on remaining) so broken on this issue in our country. But I do have my own interesting story/perspective to add.
In my late 30s, I began to experience a number of problems that eventually were diagnosed as rheumatoid arthritis. As a person who had always been fairly healthy and was concerned about over medicating, I spent several years using the basic and inexpensive treatments but seeing few improvements in my symptoms.
I finally decided to go forward with a more aggressive treatment, giving self-injections of the biologic Humira. It took some time, but after a year on this drug, I was 90% of my former self. After several years, I was at 100%, and even saw improvements on things that no one had ever suggested were connected to RA (canker sores, pimples, even finger nail health).
The economics of this drug are crazy though. The routine I am on, and the one I understand to be most common, is two injections per month. The cost for the drug? About $60,000 per year!
Of course, as one of the people fortunate to have health insurance through an employer, I don’t pay that. Still, ignoring my deductible, my co-pay is $95 per month. A steal compared to the cost of the drug, but quite a number to add to my budget for the rest of my life.
Here’s the part that really blows my mind, though. Some foundation, run by Abbott (the maker of Humira), enrolled me in an assistance program. I didn’t have to do anything to enroll, and honestly my finances are comfortable enough that I could cover the co-pay easily enough. With the co-pay assistance, I pay $5 per month.
Said another way, a foundation pays $90 on my behalf to make sure that my insurance company will pay $5,000 to the manufacturer who created that foundation.
I am probably missing lots of other grift and inefficiencies built into this system. But it is remarkable to me that someone has figured out a way to extract payment of 1000 times the multiple that most of the drug consumers can pay.
Pretty bleak when everything depends on pure capitalism. Late capitalism kills.
I’m late to this, but just wondering, does anyone have a link to why Trump was considered basically bankrupt before the election? I remember Marcy mentioning it before and I’d just like to read some evidence of it.
Welcome to emptywheel. I’ve deleted your earlier duplicative comment. I can’t find a post by Marcy which says explicitly that Trump is/was bankrupt (beyond the several bankruptcies we all know about), but she did write a post in which The Apprentice TV show’s turd polishing effect figures largely.
A topic near and dear to my heart. I work in the belly of the beast as an MD in an ICU. Parent was an economist.
1) The supply demand curve implies a non-functioning market. For pricing to reflect demand and supply there must be competition. This is prevented by patents and collusion among suppliers. Patent laws have been distorted over the years and products and be protected for excessive periods of time. Insulin pricing implies supplier collusion. Jeff Bezos like to say your margin is my opportunity for profit. If insulin is profitable when cheap, then 400% later it is an opportunity. The lack of a new supplier suggests collusion. DOJ investigation? Aren’t there laws on the books about profiteering? Any JD wish to comment?
2) Medical care is relatively price insensitive. Think not? Shop around for you next elective operation. Say a knee replacement. Singapore may be cheaper, Mexico even cheaper, and Albania a real bargain. End up with a complication of a knee replacement done in Singapore and then what?
3) Quality is very hard to measure. A nearby hospital is higher rated than mine for one of the principle diagnoses I treat, yet they sent their more difficult cases to us. We use a national firm to risk adjust for outcomes. I tried to find how they validate their data, all they would provide was a chart showing their data as measured by quartiles was highly correlated to their data as measured as a percentage (mathematical coupling of data in the worst way.)
4) Payment for quality ends up being a means of punishing the poor. How? Well off systems have fleets of reviewers to massage the data. Poor rural and inner city hospitals do not. An example, ventilator associated pneumonia is a common complication of being on life support. It occurs roughly at a rate of 1% per day on life support and no scientific study has shown anything greater than a 50% reduction no matter how hard an ICU tries. Yet there are systems out there making claims like 700 days with out a ventilator associated pneumonia. Poor hospitals do worse on the quality measure, get paid less, making keeping the doors open even harder.
5) Quality measure frequently have severe unintended consequences. My system wants to judge my performance based on mortality. This would be easy for me to game. Never mention hospice care or comfort based palliative care and sent everyone possible to an LTAC (long-term care facility.) Punt all the difficult decisions in very sick patients nearing the end of life down the road (I would never do this). Surgeons face similar issues as they get rated on surgical outcome. It is easy for them to refuse as patient saying not a candidate, they will die on the table. But maybe you want to take that 5% chance at life with a risky operation. In some areas high risk patient are not given the choice.
6) The cost of doing anything must be weight averaged over all payers. Most of what a hospital does loses money. The highest payers are the target for the ridiculous prices quoted. Just a few golden commercial payers can make up for the less profitable payers. Self pay is the hospital killer, too much and it’s difficult to keep the doors open.
7) Most choices of provider and hospital are based on geography. Dial 911 and they will take you to the nearest hospital. No discussion. End up needing to be admitted and ask to be transferred to your choice and it in some cases may happen.
Thank you so much for taking the time to comment.
This: The supply demand curve implies a non-functioning market. Exactly. If a market is a conversation, there’s no discussion here.
Medical care is relatively price insensitive. Yup, makes absolute sense since medical professionals have beaucoup tuition to recoup and malpractice insurance to pay for everything they do. Yet my GP was relatively price stable over the 30 years I was with his practice.
Quality is very hard to measure. Just as you explained, not to mention the annoying variation in humans and their qualia.
How do we fix this? I don’t expect you to answer that. But it certainly can be done better than it is here, other countries prove it. The $3.5 trillion we will spend this year on health care for those who have some means to pay tells us we must do something.
Thanks again.
It really was an excellent contribution.
GREAT observations. Thank you.
So I paid my dues with a hitch in the navy and use the VA for my total health care needs (except dental, damn it). It’s been consistently good, not great but good. My heart meds cost a max $15.00 copay. Of course this can’t stand and Trump and others think adding more bureaucracy and a large profit margin will provide cheaper, better care. Even with the VA and Kaiser model, national health care will not happen in my life.
Spent my time in training at a VA. Above average care for all. The vets were appreciative and great to take care of. Worst care? Often the rich who end up with the docs with pinstripes and a nice smile. But the VA uses MDs and facilities like mine when the going gets tough.
Thanks Rayne. Broken system. A friend of mine had encephalitis. She survived, recovered and went bankrupt. The hospital and drugs costs were enormous. Not only did she have to learn to walk and talk again, she also had to rebuild her credit and finances. Plus the top notch doctor misdiagnosed her condition.
Report about individuals going to Tijuana for cheaper prescription drugs.
https://www.npr.org/sections/health-shots/2019/02/11/691467587/americans-seek-cheaper-meds-in-mexico
Pharma greed. Benefiting share holders rather than patients.
I realize this thread is not about Firdapse per se, but it may still be helpful to understand some of the backstory as to how Firdapse came to be so watch this:
https://www.youtube.com/watch?v=bowqxIBI15k
From the video, note how the IP leading to Firdapse, which was purchased not from Jacobus, but (presumably) from the original European source (unsure about the details), lead to the FDA awarding approval and seven year exclusivity to Catalyst, but that also prevents Jacobus from making and even providing their variant for compassionate use.
As far as other drugs/treatments that seem to fit this predatory model I recall the EPI pen might fit this topic.
Corrections welcome…
sooner or later, someone will violently react to inelastic demand insulin prices and we’ll have regulation
Already have. A 26-year-old man died because he couldn’t afford enough insulin. I imagine there are old victims out there but they may be ignored because of their age and anticipated mortality.
How many more 20-somethings do we need to lose before something changes?
A few points re “vertical demand” and insulin–which is about as vertical as it gets, something I know about having been Type 1 diabetic since 1983.
* In broad terms, yup, the price gouging is outrageous. One thing almost all T1s do is hoard the stuff. Unless you know what it’s like to be in a situation where, if your drug runs out, you’ll be going into a really unpleasant death spiral within 24-36 hours (DKA, or Diabetic Keno-Acidosis, not fun), you can’t understand how paranoid you get about this stuff. Thing is, the amount of insulin you need per day varies widely by what you’re eating, so what we do is have our scrip written for the max amount we might use, which lets you build up a reserve in case of the Zombie Apocalypse or other supply crises. Recently this allowed me to help out a recently diagnosed T1 friend who didn’t know about doing this, and who hit the “donut hole” where she was going to have to shell out $1200 she didn’t have for the stuff she needed to stay alive. I had extra vials of Novolog I could give her from my stash, so crisis avoided, but you can’t imagine how helpless you feel–she was seriously panicked until I learned of her situation and was able to help out. This kind of thing goes on among members of the Tribe all the time; there are Facebook pages dedicated to these exchanges. But it’s not a rational solution; it’s a band-aid on a big problem.
* Insulin Isn’t One Thing. In the late 90s, the so-called “analog” insulins most of us use made possible the standard Multiple Daily Injection (MDI) regimen most of us were trained on (and a very helpful precursor to using a pump, though that’s still a minority). In MDI you inject a flat-effect daily insulin like Lantus that just keeps you at a steady level that prevents DKA, then use a fast-acting insulin like Novolog or Humalog for meals, dose calculated by an individual formula based on # of carbs in the food, your insulin sensitivity ratio etc. These are the insulins whose prices have gone from $20/vial to $350/vial since they came on the market. They are produced in a very different–and obviously patentable–manner from the Lente stuff people used up until roughly the 70s, or the Regular and NPH insulins that became standard in the 80s-90s before modern MDI.
* Rationing. Notably, R/N insulins are still available without a prescription from Walmart for a reasonable OTC price. But despite the “Walmart” insulins, people are dying because of unaffordable insulin. Typically it’s 20-somethings who are suddenly dropped off their parents’ benefit plans and have to fend for themselves, and who are working gig-economy “jobs” or other tenuous employment circumstances that don’t provide insurance and are facing staggering deductibles under ACA options. When these cases get reported, you’ll often hear people argue that hey, you can always buy Walmart insulin for cheap, so what’s the big deal. The big deal is that 1) they are not the same as Lantus/Novolog. The crazy thing about T1, something that goes against the whole grain of the medical profession, is that it requires patients to dose themselves with a drug that can render them unconscious or kill them, based entirely on their own calculations without direct medical supervision, and they have to do this multiple times a day for the rest of their lives. Virtually nothing else this dangerous gets prescribed like this and there are all kinds of ways in which the FDA and the medicos signal their discomfort with it, but there’s no way around it. Point is, ALL of these different insulins require training to use safely, Figuring out your I:C and Sensitivity ratios, what your basal dose is–all that takes a lot of testing and incremental adjustments under close supervision, can take a few weeks to get dialed in, and being trained on Lantus-Novolog MDI does NOT transfer in any simple way to using the older insulins. Suddenly switching to something that works in a whole different manner is not at all straightforward, and if you’ve ever experienced a severe hypo episode, it’s scary–you can get very gun-shy about it. And these older ones are harder to use. It takes some expertise to use them safely, and if you’re uninsured and struggling financially, that expertise is not necessarily ready to hand. 2) it’s a very different regimen in terms of quality of life. I was on R/N for 20 years and used to refer to it as Eat Now or DIE! They peak at separate times, with the effect curves crossing several hours out from when you take them, which absolutely constrains your daily existence around your expectation of when they’re going to hit, and all kinds of factors can interfere and throw those expectations off. Sitting in a meeting, driving a car, walking down the street and having your vision suddenly go blank in the center–the first sign of a bad hypo in my case–is y’know, kinda scary, not to mention it makes actually DOING anything about it rather difficult. That kind of thing was much more common for me and many of us on R/N. I hated being on that stuff, but the alternative was, y’know, death.
* Which is to say that, price competition between R/N and standard MDI isn’t very competitive. It’s not nothing, there are even some people who actually prefer the old stuff, but few dx’d in the last 20 yrs were ever trained on it, and for 90% of us it’s a very different world. It’s scary to have to do inject yourself with this stuff to begin with, you can always make mistakes—everyone gets it wrong sometimes–but the modern insulins make it so you can actually delay a meal or deal with unscheduled exercise (having to run to make a bus, e.g.) without worrying quite so much that you’re going to end up in a scary situation. R/N, not so much.
* So where are the “generic” competitors for modern insulins? For various technical reasons it’s very difficult to come up with off-patent “biosimilar” drugs. The ONLY one that exists so far, Basaglar, is a biosimilar for the other basal insulins like Lantus. It’s also made by the same company–Lilly–that makes Lantus. So “competition” isn’t really the right word. They sell it for a bit cheaper, but only a bit. And it’s only one piece of the MDI equation; you still need a fast acting insulin. And no help at all for us pump users, for whom the fast-acting (e.g. Novolog, Humalog, Fiasp) is ALL you use.
* PBMs. Pharmacy Benefit Managers. The thing is, it’s not just Big Pharma doing Bad Things, here. A lot of us think the PBM layer is the real culprit in insulin price gouging, both in inflating prices and disguising what the actual prices are, so that each party in the tripartite scheme can lay blame on one of the others to avoid consequences. It’s basically an invoice-fraud scheme, tweaked to look legit, where the gap between the reported price and the actual price goes to fatten the bank accounts of everyone in on the scheme. A lengthy subject and I’ve already used far too much space, but it’s really essential to the whole problem. This Hagens-Berman lawsuit covers the details quite well: https://www.businesswire.com/news/home/20170130005967/en/Hagens-Berman-Insulin-Manufacturers-Hit-Class-Action-Lawsuit
This is a repost – the first one vanished.
I believe that big pharma’s lobbying efforts have much to do with the high costs of our drugs. For example, I have eye drops that cost me about $600/m (Bronze plan costs) and there is no generic available in this country. Two years ago my opthamologist was hoping a generic would come onto the market, but Allergen’s lobbying efforts killed that idea. (I’m repeating what my doc told me.) Apparently they felt they hadn’t recouped all of their initial investment, hence the need for continuing their monopoly on the drug.
According to Citizens for Responsibility and Ethics in Washington, (excerpt below)
The pharmaceutical industry has had a robust and organized lobbying operation on Capitol Hill for years. Over the last decade, Big Pharma has spent roughly $2.5 billion lobbying the federal government on a broad range of issues, including efforts to limit drug prices. The industry allegedly promised to support President George W. Bush’s 2006 Medicare Part D plan on the condition that the Centers for Medicare and Medicaid Services (CMS) would be forbidden from negotiating for lower drug prices. In 2009 and 2010, during the negotiations and horse trading leading up to the passage of the Patient Protection and Affordable Care Act, more commonly known as “Obamacare,” the industry allegedly made sure that the new law would not include any proposals that would reform how prices are set for prescription drugs. These types of results don’t come cheap: in 2017 alone, the pharmaceuticals and health products industry employed more than 1,400 lobbyists and spent more than $277 million lobbying the federal government, making it one the strongest special interest groups in our nation’s capital.
The industry’s lobbying efforts are spearheaded by PhRMA, which is led by Stephen Ubl, a former biotech executive and lobbyist. From 2011 to 2017, PhRMA spent an average of $19.9 million lobbying the federal government each year. In addition to PhRMA, other industry groups, like the Biotechnology Innovation Organization (BIO), a trade group representing biotech companies, also spend money on lobbying. In 2017, BIO spent more than $9.3 million lobbying the federal government on issues including drug importation, Medicare Part D, the 340B drug discount program, and orphan drugs which are medications for rare diseases.
http://www.citizensforethics.org/a-bitter-pill-how-big-pharma-lobbies-to-keep-prescription-drug-prices-high/
(Note to moderator:I hope the excerpt and link are done correctly.)
[FYI, comments with multiple links go into moderation and may take a while to clear. Your first comment which this one duplicates has been deleted./~Rayne]
Got it! Thank you, Rayne.
If I understand the tax laws, corporations can subsidize health (sickness) insurance and neither the company nor the employees get taxed on the subsidy. What would happen if that tax loophole went away?
@drmyk February 12, 2019 at 3:10 pm
You’re talking to someone with a background in engineering and computer science. My only question was “what’s the half-life?” – I knew why they were doing it (they wanted a good shot of where the cancer was, and whether there were any other spots) and the scans picked up a couple of other things that weren’t going to show up any other way, one of which is immediately relevant to my health, and the other is longer-term. I’m not going to complain about that, except for not getting to see the pictures myself – and the PET scan really needs 3D displays.
Doctors don’t really like doing tests for no reason – all of mine seem to prefer doing without as much as possible – but they will order tests they think are necessary.
Now medical-testing companies – there’s another profitable business: they charge several times what it actually costs to process the tests. (No way is an a1c test going to cost them $70 to process – but that’s what they’re charging me.) Another area that needs to be looked at – and all the big testing companies are very much for-profit.
Well over 80% of health problems are caused by health behavior (Univ of MI, Public Health). At first glance, one thinks, it’s the fault of the “individual” but the human identity is a social one – even diets and “tastes” are socially engineered by billions of dollars spent on marketing & advertising products. Bad foods are cheaper. Good foods are costlier. EBT at McDonalds. Cheap Soda. It used to be far more expensive. CORN SYRUP in everything v. sugar. See the obesity correlation? Preservatives cause plaque on the brain. Dementia, Alzheimer’s, Type II Diabetes. The high cost of cheap foods gunning for “long shelf life” vs. human life is long ignored.
Forget “food deserts”…we’re talking everywhere. If you want to look at the killer, the dark mirror is available in any supermarket aisle. “It glitters like a morgue”. Go ahead think outside the box in your cubicle.
Big pharma is bad, but Big Food or Big Agra? (e.g. One gallon of H20 for one almond) is just as bad.
I’ve been on several expensive drugs that are toxic; they kill you to save you they say, but they’re killing me for a profit. Welcome to this American Life where SURPRISE suddenly “supply & demand” bullshit isn’t hashing out for gasoline since we’re at war. It’s hush money payments we paid to Russia and SA to play nice. Now that it’s all gone to hell no gas spikes in winter or summer or BS holidays. THINK. REMEMBER.
Wake up ppl. Someone’s bartering with our lives and they’re losing badly. IC that’s you – I’m talking to…
I don’t want to meet whatever it is you’re taking.
I love Rayne and these posts! I love to see these topics being discussed in the open!
I’m new to this site but love your recent posts!!!!
Looking forward to your future posts!
Since I know Rayne is freshly-stocked up on the Heavy Duty, I’ve got a new tinny topic:
Why’d Boehner _really_ get pushed out/resign (and we all know Ryan’s budgetary wizardry wasn’t it). Started re-thinking it at end of here, cued by summer 2015 IC report to then-Gang of Eight (plus other stuff we’re now well-aware of: NRA RU GOP RT acronym hell). Reminders re Boehner’s outspoken stances against RU’s Sovietism ahead of Putin re-election, RU sanctioning him (visa-banned him along with McCain), etc.
Sad foil jokes aside, really, because I suspect this is a viable topic as regards the long-game. I had all but forgotten about the timing of this leadership turnover, largely because in Trump years it feels like 2015 was ten years ago.
I don’t think this topic is separate from the Trump-Russia topic, in the same way that Butina-NRA isn’t separate. NRA money funded media buys directly or indirectly solely to the benefit of GOP candidates up and down the ticket after 2010, and through 2016. Voters who chose a GOP senator didn’t crossover and vote for Clinton at the top of the ticket and vice versa; the social media and commercial ad campaigns ensured linkage.
I also don’t think RU was stupid enough to put all their eggs in one fallible basket. A 70-plus-year-old dude with a lot of really bad habits wasn’t enough to ensure the sanctions were lifted.
Yeah, seeing his name, it really hit me over the head with both ~ “Oh, now this overthrow makes more sense’ and ~’the overthrow makes more sense of Trump-Russia.’ It pulls together the long-game strands quite nicely.
I’ve also been musing Boehner’s hatred of Ted Cruz,* and the Cruz-backing Mercer/Schweizer efforts. (In another duh-to-self moment) I had commented on one of Marcy’s Joule attack posts that we would be in much worse shape now possibly had Cruz won, because all of the current-day hard-right -isms, rights-stompings, (NATO-chipping, RU-hugging, etc.) would instead have the patina of normative civility. Trump’s erratic incompetence at least helps to see the crazy.
*LOL, hatred of Cruz is a highly non-specific sign
Rayne,
Ty for this thread. “it was illegal to base an exchange on forfeiting every claim to rights including one’s life; we prohibit extortion.” My B school taught ethics and logic. Quote above advises legal remedy for crime of extortion. Respect, Dignity, Autonomy are values that if held make extortion a really hard reach. My oncologist looked me in the eye and told me “I can’t cure what you have”. Ok. “But we can fight what you have”. Vertical curve meet demand. Catastrophic disease is mainly financial catastrophe in US vertical demand model. Background simplification. Otto Warburg received Nobel Prize 1931 for correctly identifying the difference between Malignant cancer and all non—malignant cancers. Malignant cancers intra-cellular method of respiration doesn’t utilize mitochondria. Instead malignant cancer cells breathe by consuming 600 times more sugar than any adjacent cells breathing with mitochondrie. PET scans use IV contrast of very short half-life radioactive sugar. Malignant cancer cells consume the radio-labeled sugar to breathe. If a cancer patient gets a PET scan any malignant tumors present will show up like Christmas tree lights inside the body. I’m a survivor and I’ve seen my PET scans full of lights and miraculously my PET scans dark. Healthcare is a human inalienable right. Here in US; well this thread is addressing the financial challenges opposed to the right to healthcare.