Ebola Outbreak Receding in Liberia, Still Strong in Sierra Leone
Back in late September, the press had a field day with a mathematical model developed by CDC that estimated that if left unchecked, the Ebola outbreak in West Africa could wind up infecting over 1.4 million people. Almost missed in the hysteria over that high number was the fact that this same model predicted that even with key public health measures (patient isolation, monitoring of at-risk population who had contact with infected people and safe burial practices) falling short of 100% implementation, the outbreak could be brought under control around January of next year.
Word has been leaking out for a while now that the rate of new Ebola infections in Liberia is falling. Reports in the Washington Post on October 29 and November 3 told us as much. A chart in the WHO Situation Report for November 5 drives home just how dramatic the decline in new cases has become:
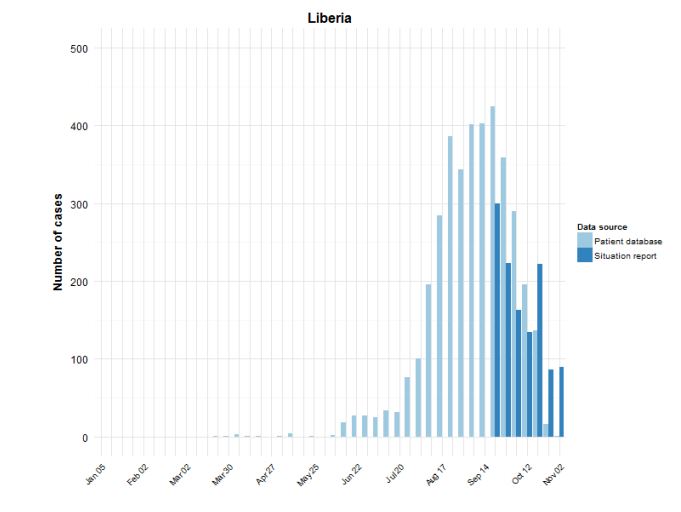
WHO Ebola Situation Report November 5, 2014
As can be seen in the chart, the rate of new infections for the two most recent weeks is less than one fourth the rate at the peak of the outbreak. Unfortunately, the news for Sierra Leone is not as good. While the rate of new infections may be leveling off, it is not yet falling appreciably:
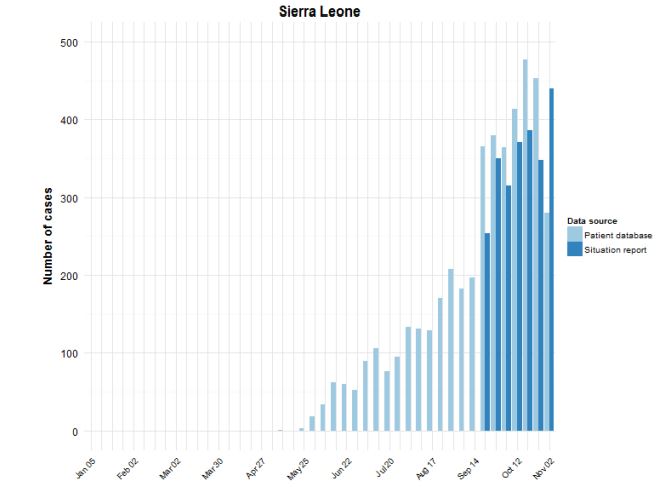
WHO Ebola Situation Report November 5, 2014
Digging into the WHO report a bit further, we can find some evidence for how this dramatic drop in new cases has been brought about. We see that 52% of cases are now isolated. The WHO target for December 1 has been set at 70%, with a target of 100% by January 1. When it comes to management of dead bodies, though, the December 1 target has already been surpassed. WHO reports that 87% of the dead are being “managed in a safe and dignified manner” while the targets were set at 70% for December 1 and 100% for January 1. Also, although no benchmarks are reported, WHO states that 95% of registered contacts were reached daily (although in the text of the report, there are suggestions this number may be somewhat overstated).
It should come as no surprise that progress in implementing these basic measures has had a huge impact on bringing down the rate of new infections. It fits perfectly with the CDC mathematical model and it also addresses the known biology of Ebola infections. Patients are most infectious at or near death, so establishing safe burial practices is vitally important. Conversely, identifying infected individuals through daily monitoring of the at-risk population and then isolating infected individuals once symptoms begin means that far fewer people are exposed to people producing large amounts of virus.
Sadly, those who remain exposed are the health care workers who are providing care to those who are infected. Despite shortages of equipment and supplies, WHO and other organizations are doing their best to overcome those shortages and to beef up training to reduce risk to these brave people on the front lines in the work to control the virus. As of this November 5 report, 546 health care workers have been infected, with 310 of them dying. Only four new infections were reported for the week ending November 2, so it is hoped that this rate is also dropping.
Had the alarmists who insisted that this was a new super-strain of Ebola capable of airborne transmission (or even a strain developed in a bioweapons laboratory), it is doubtful that these basic public health measures would have had such a dramatic impact on the rate of new infections. Perhaps those folks can go back to railing about chemtrails or the evils of vaccines, because basic boring science appears to be on the road to controlling the current outbreak before all of mankind succumbs.
In the meantime, we are at about two weeks into the three week incubation period both for anyone “exposed” by Craig Spencer or for Kaci Hickox (or anyone she “exposed”) to show symptoms. No reports of transmission so far, and the odds of any cases showing up are dropping very rapidly from the already very low levels where they started.
The clear conclusion is that public health care infrastructure at least to the level of Senegal and Nigeria is effective in quickly stopping an ebola epidemic. That means that the efforts to extend that infrastructure to countries like Guinea, Sierra Leone, and Liberia — an ironically to Spain and the United States, beset by austerity fever — are critical to US national security in the broadest sense.
And the failing in the United States was the “public” part of public health infrastructure. The fallacy of thinking that health is exclusively an individual financial responsibility.
SCOTUS has agreed to hear a case on the insurance mandate this session. That means that the four GOP-T justices want to destroy the ACA.
The straw-manning of THE STRAIN THESTRAINTHESTRAIN is quite irrationally defensive. As if it were alarmism to ask, What exactly were Chris Bishop and Tom Geisbert doing there? Don’t you want to see their TORs and deliverables? Hear what they think at Njala U.?
Why fixate on the strain, when absence of genetic modification proves nothing either way? As we know, Anthrax was not genetically engineered, or especially virulent, and it worked well enough to make Daschle and Leahy roll over for the PATRIOT Act.
“…it is doubtful that these basic public health measures would have had such a dramatic impact on the rate of new infections. Perhaps those folks can go back to railing about chemtrails or the evils of vaccines, because basic boring science appears to be on the road to controlling the current outbreak before all of mankind succumbs.” An interesting blend of total non sequitur and government-issue derision, exactly what the behavioral science research describes.
The US government continually breaches the Biological Weapons Convention. Were they doing it in Kenema too?
.
The Strain, The Strain, The Strain is important precisely because analysis of it and its DNA sequence puts a lance right through the heart of your little conspiracy. Well, maybe I shouldn’t call it little, since that conspiracy made the top 5 falsehoods list on Ebola.
.
The Ebola genome is small enough that the known lab isolates have all been sequenced. And, surprise, surprise, the earliest samples from this outbreak all fit nicely into the overall picture of Ebola circulating in the wild but don’t line up with any previous isolates.
.
And there’s one more little nugget in the work on that early sequencing. The epidemiologists have worked back through the outbreak. The first known patient was a toddler who died in December, 2013. That happened in the small village of Meliandou, Guinea. A look at the map puts that spot at 191 km (about 120 miles!) from your Kenema, Sierra Leone ground zero.
.
And yes, if you follow the DNA analysis on the anthrax outbreak, that is where you catch the government in its lies. That sequence did line up with lab samples. But those samples belonged to Bruce Ivins, who very clearly could not have made the attack material acting on his own. The FBI hounded this innocent man quite literally to his death. I don’t hesitate to call out government bad acts. Quite simply, this Ebola outbreak is not one and continuing to claim that it is flies in the face of science and human decency.
Argumentum ab auctoritate from an unsourced blurb that misrepresents Boyle’s contention as right-wing Soros/Gates hype. Very convincing. Extra points for the whiny quote! Imagine how he would have whined if Politifact had asked for TORs and deliverables. Six hundred authors beavering away to reach the er, ah, presumed first fatality. One day you’ll learn that scope is a marvelous thing.
Were US contract staff supporting disease surveillance and control? And was ebola one of the priority and epidemic-prone diseases given case definitions per WHO/UNHCR recommendations? These are easy yes-or-no questions. When did US staff gain access to indigenous ebola samples? To find that out you’ll have to ask not the scientists but third-country attachés.
Your last sentence would be great with an animated waving-flag GIF and some audio doo-doodoo. When you’ve spent as much time there as I have, then you can impugn my human decency.
.
Oh my.
.
First, the rules here are to use one email address for posting and stick to it. Use a fake one if you want, but stick with it.
.
And talk about deflection. I notice you didn’t bother to address the fact that the outbreak started a VERY long way from where it had to for your theory and you have to go to undeclared lab strains to fit the inconvenient DNA data.
.
Oh well. It’s time for football for me. Thanks for playing and enjoy the next thing you concoct.